고중성지방혈증으로 인한 급성췌장염과 다른 원인으로 인한 급성췌장염의 임상적 차이에 관한 연구
Differences in Clinical Features between Hypertriglyceridemia-Induced Acute Pancreatitis and Other Etiologies of Acute Pancreatitis
Article information

Abstract
배경/목적
본 연구의 목적은 고중성지방혈증에 의한 급성췌장염(hypertriglyceridemia-induced acute pancreatitis, HTGAP)의 임상적 특징을 담석성 급성췌장염(biliary acute pancreatitis, BAP) 그리고 알코올성 급성췌장염(alcoholic acute pancreatitis, AAP)과 각각 비교해 보는 것이다.
방법
2014년 1월부터 2018년 12월까지 대구가톨릭대학교병원에 입원한 급성췌장염(acute pancreatitis, AP) 환자의 의무기록을 후향적으로 조사하였다. 급성췌장염의 중증도와 국소합병증은 2012년 발표된 애틀란타 분류 개정안에 따라 평가하였다. 전신합병증은 수정된 마샬 점수 체계에 따라 평가하였다.
결과
총 610명의 AP 환자 중 BAP, AAP, HTGAP 환자는 각각 310명(50.8%), 144명(23.6%), 17명(2.8%)이었다. HTGAP 환자를 BAP 환자와 비교하였을 때, HTGAP에서 중등증 급성췌장염(moderately severe acute pancreatitis, MSAP) (64.7% vs. 28.1%, p<0.001)과 중증 급성췌장염(severe acute pancreatitis, SAP) (17.6% vs. 5.5%, p<0.001)의 비율이 높았다. 또한 HTGAP 환자들이 국소합병증이 더 많았고(76.5% vs. 26.8%, p<0.001,) 재발률 또한 더 높았지만(52.9% vs. 6.5%, p<0.001) 전신합병증은 유의한 차이를 보이지 않았다(23.5% vs. 11.6%, p=0.140). 반면, HTGAP와 AAP는 질병의 중증도(MSAP 64.7% vs. 63.9%; SAP 17.6% vs. 6.9%, p=0.181), 국소합병증(76.5% vs. 67.4%, p=0.445), 재발률(52.9% vs. 32.6%, p=0.096), 전신합병증 (23.5% vs. 11.5%, p=0.233)에 있어 유의한 차이를 보이지 않았다.
결론
HTGAP는 BAP보다 질병의 중증도가 더 높고 국소합병증 발생이 더 많으며 재발률 또한 더 높았다. 그러나, HTGAP와 BAP의 임상 양상은 유의한 차이를 보이지 않았다.
Trans Abstract
Background/Aim
The aim of this study was to compare clinical features of hypertriglyceridemia-induced acute pancreatitis (HTGAP) with those of biliary acute pancreatitis (BAP) and alcoholic acute pancreatitis (AAP), respectively.
Methods
Medical records of patients with acute pancreatitis (AP) who were admitted to our institution from January 2014 to December 2018 were retrospectively reviewed. Disease severity and local complications were evaluated according to the 2012 Revised Atlanta Classification. Systemic complications were evaluated according to the Modified Marshall Scoring System.
Results
Of the total 610 patients with AP, those with BAP, AAP, and HTGAP were 310 (50.8%), 144 (23.6%), and 17 (2.8%), respectively. Compared with BAP, HTGAP showed higher proportion of moderately severe acute pancreatitis (MSAP) (64.7% vs. 28.1%, p<0.001) and severe acute pancreatitis (SAP) (17.6% vs. 5.5%, p<0.001). And HTGAP showed more local complications (76.5% vs. 26.8%, p<0.001) and higher recurrence rate (52.9% vs. 6.5%, p<0.001), but there was no significant difference in systemic complications (23.5% vs. 11.6%, p=0.140). Contrarily, there was no significant difference between HTGAP and AAP with respect to disease severity (64.7% vs. 63.9% in MSAP and 17.6% vs. 6.9% in SAP, p=0.181), local complications (76.5% vs. 67.4%, p=0.445), recurrence rate (52.9% vs. 32.6%, p=0.096), and systemic complications (23.5% vs. 11.5%, p=0.233).
Conclusions
HTGAP showed higher disease severity, more local complications, and higher recurrence rate than BAP. However, there was no significant difference in clinical features between HTGAP and BAP.
서 론
급성췌장염(acute pancreatitis, AP)은 췌장의 염증성 질환으로, 세계적으로 10만 명당 13-45명의 유병률을 보인다[1]. AP 환자의 대부분은 양호한 임상 경과를 보이지만 10-15%는 괴사성 췌장염으로 진행하게 되고, 장기부전이 지속될 경우에는 사망률이 15-20%에 이른다[2]. AP의 가장 흔한 원인 두 가지는 담석과 음주이지만, 고중성지방혈증(hypertriglyceridemia, HTG)도 잘 알려진 원인이며 전체 AP의 1-10% 정도를 차지한다[2,3]. 또한 이전에 대구가톨릭대학교병원에서 수행한 대구·경북지역의 후향적 다기관 연구에 따르면, AP의 병인으로 음주가 41.5%, 담석이 33.6%, 특발성이 13.0%, 고중성지방혈증이 1.4%를 차지하였다[4].
HTG가 AP를 일으키는 기전은 아직 명확하지 않으나 중성지방이 지방분해효소(lipase)에 의해 분해되어 유리지방산이 생성되고, 생성된 유리지방산이 세정제 성질을 갖는 미셀 구조(micellar structure)를 이루어 췌장 선방세포와 모세혈관에 손상을 준다는 가설이 가장 유력하다[5]. 그리고 고중성지방혈증에 의한 급성췌장염(hypertriglyceridemia-induced acute pancreatitis, HTGAP)이 다른 원인에 의한 AP보다 중증도가 높고 합병증이 더 많이 동반된다는 보고들이 있으나 아직 확실한 결론에 이르지는 못하고 있다[3,5]. 따라서 본 연구에서는 HTGAP의 임상적 특징을 담석성 급성췌장염(biliary acute pancreatitis, BAP) 그리고 알코올성 급성췌장염(alcoholic acute pancreatitis, AAP)의 임상적 특징과 각각 비교하여 알아보고자 한다.
방 법
1. 연구 형태 및 대상자
2014년 1월 1일부터 2018년 12월 31일까지 대구가톨릭대학교병원에 입원하여 치료받은 AP 환자 610명을 대상으로 후향적 연구를 진행하였다. 연구 대상자 중 BAP, AAP, HTGAP에 해당하는 환자는 모두 471명이었으며, 그 외 특발성, 자가면역성, 종양, 폐렴 또는 신우신염과 같은 다른 감염성 질환을 동반한 경우, 18세 미만의 소아 등은 제외하였다. 이에 대한 내용을 Fig. 1에 요약하였다. 그리고 환자의 인구학적 특징, 질병의 중증도, 임상 결과를 분석하기 위하여 연령, 성별, 혈액 검사 결과, 입원 기간, 영상학적 검사 소견, 현병력과 과거력, 재발 여부 등을 조사하였다. 본 연구의 진행은 2013년 개정된 헬싱키 선언의 윤리지침에 따라 수행되었으며 대구가톨릭대학교병원의 윤리심의위원회의 승인을 받았다(Approval No. CR-21-167-L).

Flowchart of the study population. ERCP, endoscopic retrograde cholangiopancreatography; BAP, biliary acute pancreatitis; AAP, acute alcoholic pancreatitis; HTGAP, hypertriglyceridemia-induced acute pancreatitis. *Other significant infections included pneumonia, acute pyelonephritis, and appendicitis.
2. 정의
AP의 진단은 다음의 세 가지 중 두 가지 이상을 만족하는 경우로 정의하였다[2]. 1) AP에 합당한 복부 통증, 2)혈청녹말분해효소(serum amylase) 그리고/또는 혈청지방분해효소(serum lipase) 수치가 정상 상한치의 3배 이상 상승, 3) AP에 합당한 영상학적 소견 그리고 HTGAP는 혈청 중성지방수치가 1,000 mg/dL 이상이거나, 500 mg/dL 이상이면서 AP의 다른 원인이 없는 경우로 정의하였다[5]. BAP의 진단 기준은 AP의 진단 기준을 만족하면서 내시경역행담췌관조영술(endoscopic retrograde cholangiography), 내시경 초음(endoscopic ultrasound), 복부 전산화단층촬영(abdominal computed tomography) 또는 자기공명담췌관조영술(magnetic resonance cholangiopancreatography)에서 담낭 담석이나 총담관에 담석 또는 담즙찌꺼기가 확인된 경우로 정의하였다[6]. 또한 담낭 담석이나 총담관에 담석 또는 담즙찌꺼기가 확인되지 않은 경우에도 AP의 다른 원인이 없으면서 알라닌아미노기전달효소(ALT)가 60 U/L 이상이면 BAP로 정의하였다[6]. 마지막으로 AAP는 다른 원인에 의한 AP가 아니면서 알코올 남용 또는 만성적인 음주력이 있는 경우로 정의하였다.
AP의 중증도는 2012년에 발표된 애틀란타 분류 개정안(Revised Atlanta Classification)에 따라 경증(mild acute pancreatitis, MAP), 중등증(moderately severe acute pancreatitis, MSAP), 중증(severe acute pancreatitis, SAP)으로 분류하였다[7]. 그리고 국소합병증은 췌장 주위 체액 고임(peripancreatic fluid collection), 췌장거짓낭(pancreatic pseudocyst) 또는 괴사가 동반된 경우로 정의하였다[7]. AP의 전신합병증은 수정된 마샬 점수 체계(Modified Marshall Scoring System)에 따른 장기부전으로 평가하였다[8].
3. 통계 분석
연속변수의 경우 중앙값과 사분위수 범위로 기술하였고 범주형 변수는 number (%)로 기술하였다. HTGAP 환자군을 BAP 환자군 그리고 AAP 환자군과 각각 비교하였는데, 연속변수는 Mann-Whitney U test를 사용하여 분석하였고 범주형 변수는 chi-squared test 또는 Fisher’s exact test를 사용하여 분석하였다. 모든 통계분석은 SPSS version 19.0 (IBM, Armonk, NY, USA)으로 시행되었다. 양측검정으로 p-value가 0.05 미만인 경우 통계적으로 유의한 것으로 판단하였다.
결 과
1. AP 환자의 기본적 특성 및 임상적 특징
연구 기간 동안 대구가톨릭대학교병원에 입원하여 치료받은 AP 환자 610명 중 BAP, AAP, HTGAP 환자는 모두 471명이었다. Table 1에 환자의 기본적인 특성에 관하여 정리하였다. 전체 AP 환자 중 BAP 환자가 310명(50.8%), AAP 환자가 144명(23.6%), HTGAP 환자는 17명(2.8%)이었다. 연구 대상인 471명의 환자를 분석하였을 때 남성이 304명(64.5%)이었고 나이의 중앙값은 59세였다. 기저 질환으로 고혈압이 있는 환자가 156명(33.1%), 당뇨병이 있는 환자가 95명(20.2%)이었다. 음주력이 있는 환자가 211명(44.8%)이었으며 104명(22.1%)의 환자에서 흡연력이 있었다. 연구 대상인 환자의 혈액 검사 결과는 Table 2에 요약하였다 . 혈청녹말분해효소와 혈청지방분해효소의 중앙값은 각각 428 U/L와 986 U/L였으며 정상 상한치의 3배 이상 혈청녹말분해효소가 증가한 환자는 274명(58.2%)이었다. 백혈구 수치의 중앙값은 10.7×103/μL였고, 혈액요소질소(blood urea nitrogen)의 중앙값은 13.5 mg/dL, 크레아티닌 수치의 중앙값은 0.8mg/dL였다 . 아스파트산아미노기전달효소(AST)와 ALT 수치의 중앙값은 각각 112 U/L와 84 U/L였다. 또한 C-반응 단백질(C-reactive protein, CRP) 수치의 중앙값은 18.6 mg/L였다.

Baseline characteristics of patients with acute pancreatitis
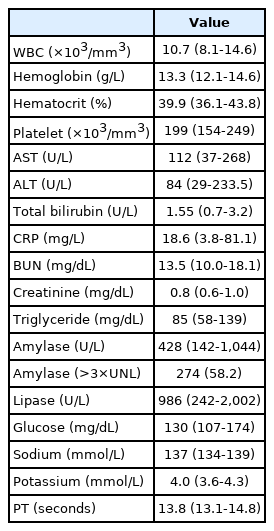
Laboratory findings of patients with acute pancreatitis
질병의 중증도와 임상 결과는 Table 3에 정리하였다. 2012년 발표된 애틀란타 분류 개정안에 따라 분류하였을 때 MAP가 251명(53.3%), MSAP가 190명(40.3%), SAP가 30명(6.4%)이었다. 합병증 발생 비율을 살펴보면, 국소합병증이 발생한 환자는 모두 193명(41.0%)이었으며 전신합병증이 발생한 환자는 56명(11.9%)이었다. 국소합병증으로는 췌장 주위 체액 고임이 161명(34.2%), 췌장거짓낭이 61명(13.0%), 괴사가 63명(13.4%) 있었다. 또한 전신합병증으로는 호흡부전이 13명(2.8%), 신부전이 54명(11.5%), 심혈관계 부전이 19명(4.0%) 있었다. 환자들의 입원 기간의 중앙값은 9일이었으며 중환자실 치료가 필요하였던 경우는 14명(3.0%)이었다. 또한, 사망한 환자는 4명(0.8%)이었고 76명(16.1%)의 환자가 재발을 경험하였다.

Clinical features of patients with acute pancreatitis
2. HTGAP와 BAP 환자의 비교
HTGAP 환자와 BAP 환자의 기본적인 특성과 혈액 검사 결과를 비교하여 Tables 4, 5에 각각 정리하였다. HTGAP 환자는 BAP 환자보다 나이가 더 젊고(37세 vs. 69세, p<0.001) 남성의 비율이 높았으나(82.4% vs. 53.2%, p=0.023) 체질량지수는 두 군에서 차이가 없었다(24.2 vs. 23.5, p=0.326). 당뇨병 가진 환자의 비율은 통계적으로 유의하지는 않았으나 HTGAP 환자군에서 더 높았다(41.2% vs. 20.0%, p=0.060). 음주력(64.7% vs. 18.1%, p<0.001)과 흡연력(41.2% vs. 13.5%, p=0.007)이 있는 환자들은 HTGAP 환자군에서 더 많았다. 두 군의 혈액 검사 결과를 비교해 보면, HTGAP 환자군에서 혈색소 수치(15.2 g/L vs. 12.8 g/L, p<0.001)와 CRP 수치(88.0 mg/L vs. 16.4 mg/L, p<0.001)가 더 높은 반면 혈청녹말분해효소 수치(190 U/L vs. 694 U/L, p<0.001), 혈청지방분해효소 수치(356 U/L vs. 1,133 U/L, p=0.004), 소듐 수치(131 mmol/L vs. 138 mmol/L, p<0.0001)는 더 낮았다.

Comparison of baseline characteristics between HTGAP and other etiologies of AP
Table 6에는 HTGAP 환자와 BAP 환자의 임상적 특징을 비교하여 정리하였다. HTGAP 환자 중 MAP, MSAP, SAP 환자는 각각 3명(17.6%), 11명(64.7%), 3명(17.6%)이었다. 반면 BAP 환자 중 MAP, MSAP, SAP 환자는 각각 206명(66.5%), 87명(28.1%), 17명(5.5%)으로 HTGAP 환자군에서 중증도가 통계적으로 유의하게 더 높았다(p<0.001). 또한 국소합병증의 비율도 췌장 주위 체액 고임(76.5% vs. 21.3%, p<0.001)과 괴사(29.4% vs. 6.1%, p<0.001) 모두 HTGAP 환자군에서 더 높았다. 췌장거짓낭(23.5% vs. 8.1%, p=0.053)의 비율도 HTGAP 환자군에서 더 높았으나 통계적으로 유의하지는 않았다. 재발률은 HTGAP 환자군에서 통계적으로 유의하게 더 높았다(52.5% vs. 6.5%, p<0.001). 반면 전신합병증(23.5% vs. 11.6%, p=0.140), 중환자실 입원율(5.9% vs. 2.3%, p=0.351), 입원 기간(12일 vs. 9일, p=0.087), 사망률(0.0% vs. 1.0%, p=1.000)은 두 군에서 유의한 차이가 없었다.
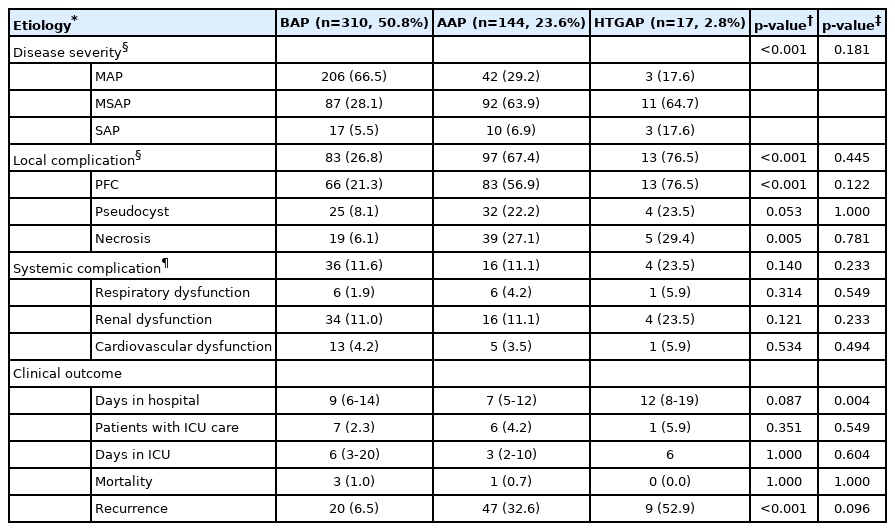
Comparison of clinical features between HTGAP and other etiologies of AP
3. HTG-AP와 AAP 환자의 비교
Tables 4, 5에 HTGAP 환자와 AAP 환자의 기본적인 특성과 혈액 검사 결과를 비교하여 정리하였다. HTGAP 환자가 AAP 환자보다 나이가 더 젊고(37세 vs. 48세, p<0.001) 체질량지수는 더 높았으나(24.2 vs. 22.2, p=0.022), 성별은 두 군에서 차이가 없었다(남성 82.4% vs. 86.8%, p=0.707). 당뇨병을 가진 환자의 비율은 통계적으로 유의하지는 않았으나 HTGAP 환자군에서 더 높았다(41.2% vs. 18.1%, p=0.055). 두 군의 혈액 검사 결과를 비교해보면 HTGAP 환자군에서 혈색소 수치(15.2 g/L vs. 14.1 g/L, p=0.022)와 CRP 수치는 더 높았고(88.0 mg/L vs. 19.7 mg/L, p=0.008) 소듐 수치는 더 낮았다(131 mmol/L vs. 135 mmol/L, p=0.032). 그러나 혈청녹말분해효소(190 U/L vs. 213 U/L, p=0.438)와 혈청지방분해효소(356 U/L vs. 622 U/L, p=0.158)는 유의한 차이를 보이지 않았다.
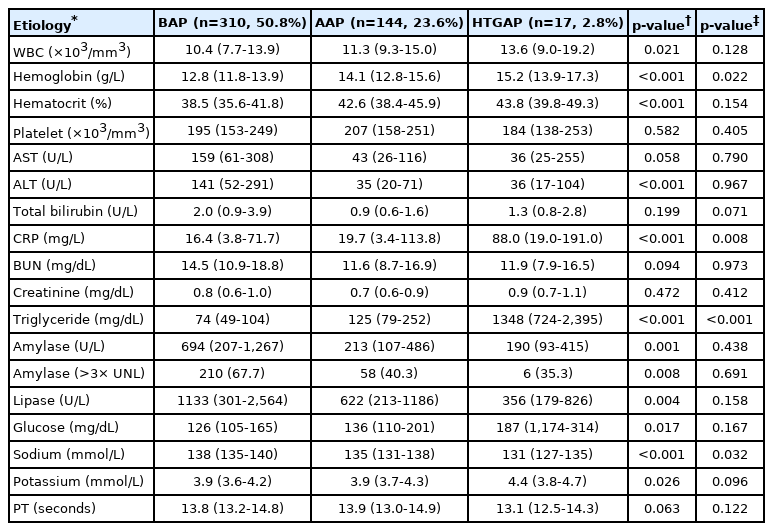
Comparison of laboratory findings between HTGAP and other etiologies of AP
두 군의 임상적 특징을 비교한 Table 6을 보면 국소합병증(76.5% vs. 67.4%, p=0.445), 전신합병증(23.5% vs. 11.1%, p=0.233), 사망률(0.0% vs. 0.7%, p=1.000), 중환자실 입원율(5.9% vs. 4.2%, p=0.549)은 통계적으로 유의한 차이가 없었다. 반면, HTGAP 환자군에서 입원 기간이 더 길었다(12일 vs. 7일, p=0.004). AAP 환자 중 MAP, MSAP, SAP 환자는 각각 42명(29.2%), 92명(63.9%), 10명(6.9%)으로 HTGAP 환자와 비교하였을 때 유의한 차이를 보이지 않았다(p=0.181). 또한 HTGAP 환자군에서 재발률이 높았으나 통계적으로 유의하지는 않았다(52.9% vs. 32.4%, p=0.096).
고 찰
HTGAP의 임상적 특징에 대해 연구한 최근 논문들에 따르면 HTGAP는 남성에서 60.0-70.2%로 좀 더 흔하고 평균 나이는 39-46세였다[9-12]. 그리고 HTGAP 환자들은 다른 원인에 의한 AP 환자들보다 당뇨병을 동반한 비율이 더 높았다(32.1-70.0% vs. 12.9-15.3%) [9-12]. 본 연구에서도 HTGAP 환자는 남성에서 82.4%로 더 많았고 나이의 중앙값은 37세였다. 이는 HTG의 임상적 특징과 관련이 있다. HTG의 유병률은 16세 이상 65세 이하의 나이 대에서 남성이 18.6% 여성이 4.6% 정도로 남성에서 더 흔한 것으로 알려져 있다[13]. 또한 HTGAP에서 당뇨병을 동반한 비율은 41.2%로 통계적으로 유의하지는 않았지만, BAP 환자의 20.1%와 AAP 환자의 17.9%보다 높았다. HTG는 인슐린 저항성과 관련이 있는데, 인슐린 저항성은 말초혈액의 지방분해를 증가시키고 유리지방산의 간으로의 유입을 증가시킴으로써 간의 초저밀도단백질(very low density lipoprotein, VLDL) 생성을 증가시킨다[14]. 또한, 1형 당뇨병에서도 절대적인 인슐린 결핍은 지방세포로부터 지방분해를 유발하여 간으로의 유리지방산 유입을 증가시킨다[14].
본 연구에서 HTGAP 환자는 저나트륨혈증을 보였고, BAP 그리고 AAP 환자들 보다 소듐 수치가 통계적으로 유의하게 낮았다. 이는 소듐을 측정할 때 물이 혈장의 93%를 차지한다는 가정하에 간접 전위측정(indirect potentiometry)을 이용하는데, HTG로 인해 혈장에서 물이 차지하는 비율이 줄어들어 가성 저나트륨혈증이 나타날 가능성이 있기 때문이다[15,16]. 또한 혈청중성지방 수치가 500 mg/dL 이상일 경우 혈청녹말분해효소 및 혈청지방분해효소 활성도 측정에 간섭을 일으켜 이들 효소가 실제보다 낮게 측정될 수 있다[5]. 본 연구에서 HTGAP 환자는 BAP 환자보다 혈청녹말분해효소 수치와 혈청지방분해효소 수치가 낮았으며 혈청녹말분해효소가 정상 상한치보다 3배 이상 증가한 환자의 비율도 통계적으로 유의하게 낮았다. 그리고 AAP 환자와 비교하였을 때 통계적으로 유의하지는 않았으나 혈청지방분해효소 수치가 더 낮았다. 따라서 HTGAP 환자를 진단할 때 혈액 검사 해석에 주의를 해야 한다.
한 체계적 문헌고찰에 따르면 HTGAP와 다른 원인에 의한 AP의 중증도를 비교한 7개의 연구 중 2개의 연구는 중증도의 차이가 없다고 보고하였으나, 5개의 연구는 HTGAP의 중증도가 더 높다고 보고하였다[17]. 그리고 HTGAP와 non-HTGAP의 중증도를 비교한 최근의 전향적 연구에서는 중환자실 입원율, Ranson 지표, 전신염증반응증후군(systemic inflammatory response syndrome), 재발률은 HTGAP에서 더 안 좋은 결과를 보였으나 사망률, 합병증 발생, 2012년 발표된 애틀란타 분류 개정안에 따른 중증도는 두 군에서 차이를 보이지 않았다[11,12]. 본 연구에서는 2012년 발표된 애틀란타 분류 개정안에 따라 HTGAP 환자군을 BAP 그리고 AAP 환자군과 각각 비교하였다. 애틀란타 분류 개정안에서는 장기부전 유무, 국소 또는 전신합병증 유무, 장기부전이 48시간 이상 지속되는 지를 기준으로 AP를 경증, 중등증, 중증으로 분류하였다[7]. 애틀란타 분류 개정안은 AP의 임상 양상에 대한 여러 연구에서 사용되었는데, 대구가톨릭대학교병원에서 수행한 대구·경북지역 다기관 연구에서는 SAP 환자가 MAP 환자보다 입원 기간이 13일 vs. 5.9일로 더 길었다[4]. 또한, 한 국제 다기관 연구에서는 SAP에서 28.4%, MSAP에서 1.5%, MAP에서 0.4%로 중증도가 높을수록 사망률이 높음을 보고하였다[18]. 본 연구에서 HTGAP 환자군은 BAP 환자군보다 질병의 중증도와 국소합병증 발생 비율이 높았으나 사망률, 입원 기간, 중환자실 입원율은 차이가 없었다. 반면 HTGAP 환자군을 AAP 환자군과 비교하였을 때 질병의 중증도, 국소합병증 발생률, 사망률, 입원기간, 중환자실 입원율 모두 차이가 없었다.
연구에 따라 이러한 차이를 보이는 이유에는 두 가지를 들 수 있다. 첫 번째 이유는 연구마다 HTGAP의 진단 기준이 일치하지 않았고 HTGAP 환자의 중성지방 수치도 차이를 보였기 때문이다. HTGAP의 혈청 중성지방 수치 기준은 500 mg/dL 이상 또는 1,000 mg/dL 이상으로 연구마다 다르게 적용되었다. 또한 Nawaz 등[19]은 중성지방 수치가 높을수록 질병의 중증도가 높음을 보고한 바 있다. 두 번째 이유는 HTGAP와 AAP의 구별이 명확하지 않다는 점이다. 본 연구를 포함한 HTGAP의 임상 양상에 관한 연구에서 환자의 음주력과 혈청 중성지방 수치를 근거로 하여 HTGAP와 AAP를 구별하였다[9,11,12]. 소량의 음주는 중성지방 수치에 미치는 영향이 적으나, 만성적인 과음은 간에서 VLDL 생성을 촉진, VLDL 찌꺼기(remnant) 및 암죽미립(chylomicron)으로부터 중성지방의 추출을 증가시켜 HTG를 유발한다[20]. 그리고 HTG 수치는 금식을 하면 72시간 내에 정상에 가깝게 떨어지기 때문에 혈액 검사를 시행한 시기가 중요하며, 복통 발생 후 24시간 이내에 검사를 하는 것이 중요하다고 알려져 있다[5]. 따라서 앞으로 HTGAP에 대한 명확한 진단 기준 확립과 더불어 엄격한 혈액 검사 조건을 적용한 대규모 전향적 연구가 필요할 것이다.
본 연구에는 몇 가지 제한점이 있다. 첫 번째는 단일기관에서 수행한 후향적 연구이기 때문에 일반화하기 어렵고, AP의 병인 분류에 있어 오류가 있을 수 있다. 두 번째는 BAP 환자들 중에는 입원 기간 중에 담낭절제술을 받은 환자들이 포함되어 있어 입원 기간에 영향을 줄 수 있다. 세 번째는 HTGAP 환자군의 수가 다른 환자군에 비해 상대적으로 적었다. 그렇지만 본 연구에서 HTGAP 환자의 비율은 2.8% 정도로 이전 보고들과 크게 차이 나지 않았으며, 471명의 환자 중 390명의 환자(82.8%)에서 입원 당시 중성지방이 측정되었는데, 이는 이전 연구의 49.9-78.0%보다 높은 수치이다[10-12].
결론적으로, HTGAP는 남성에서 더 흔하며 BAP 그리고 AAP 환자보다 더 젊은 나이에서 발생한다. HTGAP는 BAP보다 중증도가 높고 국소합병증 발생이 많으며 재발이 흔하였다. 반면, HTGAP와 AAP는 질병의 중증도, 국소합병증, 재발률에 있어 유의한 차이를 보이지 않았다.
Notes
Conflict of Interest
Jimin Han is currently serving as a deputy editor in the Korean Pancreatobiliary Association Publication Committee; however, Jimin Han was not involved in the peer reviewer selection, evaluation, or decision process of this manuscript. Tae Il Kim, Han Taek Jeong, Jeong Eun Song, and Ho Gak Kim have no conflicts to disclose.