ERCP 시술 중 발생한 십이지장 천공 상태에서 성공적으로 ERCP를 시행한 2예
Two Cases of Successful ERCP during ERCP-Related Iatrogenic Duodenal Perforation
Article information

Abstract
내시경적 역행성 담췌관 조영술 시술 중 발생한 십이지장 천공의 발생은 드물게 일어나나 사망에까지 이를 수 있는 주요 합병증 중의 하나이다. 십이지장 천공 발생시 일차적 치료로 수술적 치료가 권고되고 있으나 경우에 따라 해부학적 위치, 천공의 크기, 환자의 상태, 시술자의 숙련도 등을 고려하여 적절한 내시경적 봉합을 시도해볼 수 있다. 저자들은 내시경적 역행성 담췌관 조영술 시행 중 발생한 천공에 대하여 지혈 클립으로 일차 봉합하고, 시술을 위한 스텐트 삽입 또한 시행하여 성공적으로 치료한 증례를 보고한다.
Trans Abstract
Endoscopic retrograde cholangiopancreatography (ERCP)-related perforations of the duodenum are rare but serious complications. Some ERCP-related perforations can be successfully managed without surgery. However, the presence of duodenal perforation may lead to premature termination of the ERCP and need for additional procedure such as percutaneous biliary drainage. If the ERCP-related perforation is identified early during the procedure, primary closure of the perforation can be attempted first or after completion of ERCP. We report two cases of duodenal perforation during ERCP in which ERCP was successfully completed after primary closure of the perforation.
서 론
내시경적 역행성 담췌관 조영술(endoscopic retrograde cholangiopancreatography)은 최근 시행빈도가 증가하는 추세로 각종 췌담관 질환에서 진단 및 치료 목적으로 널리 이용되고 있는 술기이며 침습적인 시술이기도 하다. 여러 연구에 따르면 내시경적 역행성 담췌관 조영술과 관련한 합병증 발생률은 5-10%로 보고되고 있다. 이 중 천공의 경우 빈도는 1% 내외로 알려져 있으나 사망률은 10%까지 보고되고 있는 중요한 합병증이다[1,2].
저자들은 담도암이 의심되는 환자에게서 내시경적 역행성 담췌관 조영술 시행 중 십이지장 천공이 발생하였으나 시술 종료 후 지혈클립으로 치료한 1예와 췌장암 환자에게서 내시경적 역행성 담췌관 조영술 시행 중 십이지장 천공이 발생하였으나 지혈클립으로 일차 봉합 후 내시경적 역행성 담췌관 조영술을 다시 시행한 1예를 경험하였기에 문헌고찰과 함께 보고하고자 한다.
증 례
1. Case 1
89세 여자가 내원 1개월 전부터 시작된 황달로 내원하였다. 환자는 3년 전 뇌경색 및 폐동맥 색전증으로 치료받은 적이 있으며, 내원 1년 전 왼쪽 대퇴부 골절로 인하여 거동이 불편하여 타 병원에서 보존적 치료 중이었다. 계통적 문진에서 특이 소견은 보이지 않았으며, 말초혈액 검사에서 백혈구 10,750/mm3, 혈색소 8.7 g/dL, 헤마토크리트 25.4%, 혈청생화학 검사에서 아스파테이트아미노전이효소 355 IU/L, 알라닌아미노전이효소 307 IU/L, 알부민 2.1 g/dL, 총 빌리루빈 11.91 mg/dL, 직접 빌리루빈 10.09 mg/dL, 알칼리인산분해효소 2,405 IU/L, 감마글루타밀전이효소 1,505 IU/L, 탄수화물항원 19-9 879.9 U/mL로 증가되어 있었다. 내시경 초음파 및 복부 컴퓨터단층촬영에서 간내 담관 및 총담관의 확장과 원위부 담도의 협착 및 담도벽의 비후가 관찰되었으나 림프절 전이 및 원격 전이는 관찰되지 않았다(Fig. 1).
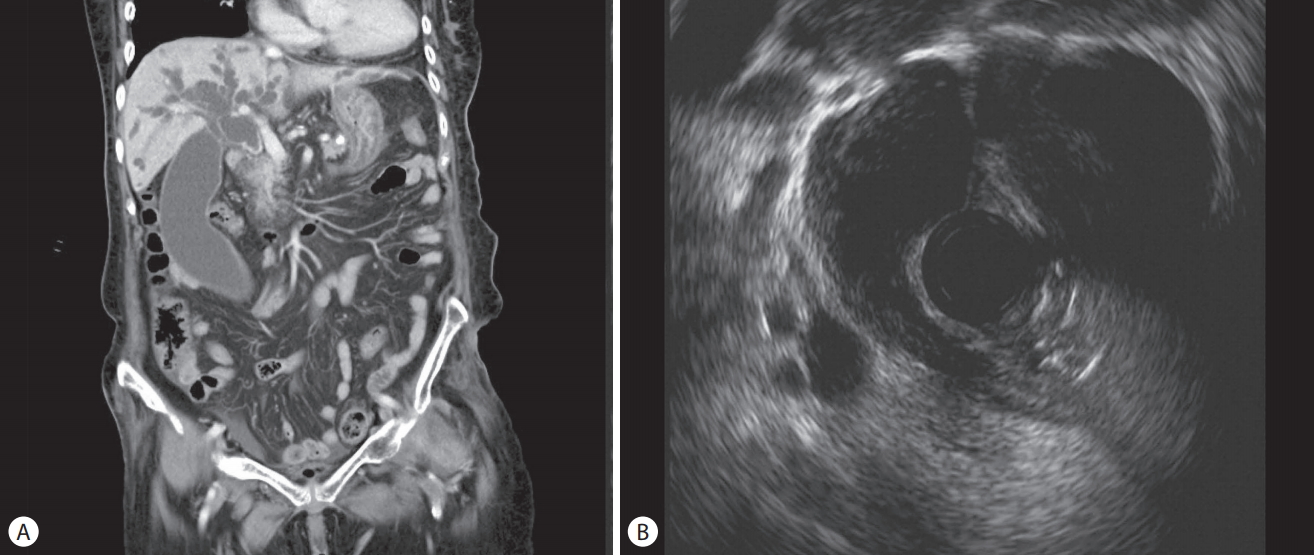
(A) Computed tomography scan (coronal view) shows periductal wall enhancement and abrupt narrowing in the common bile duct with intrahepatic bile duct dilatation. (B) Endoscopic ultrasonography image shows abrupt narrowing in the common bile duct.
원위부 담도암을 의심하여 내시경적 역행성 담췌관 조영술을 시행하였다. 내시경 검사는 십이지장경(TJF 240; Olympus Optical Co., Ltd., Tokyo, Japan) 및 상부위장관 내시경(GIF-Q240; Olympus Optical Co., Ltd.)을 사용하였으며, 시술은 모두 공기를 사용하여 이루어졌다. 십이지장경을 삽입하는 과정에서 투시 검사상 후복강내 공기음영이 확인되어 십이지장 천공을 조기에 인지하였다(Fig. 2). 천공을 인지하였으나 환자의 생체징후가 안정적으로 유지되어, 시술을 지속하였으며 담도내 플라스틱 스텐트를 삽입하여 담도 배액을 시행하였다(Fig. 3). 시술 후 십이지장경을 회수하며 십이지장 제2부의 원위부 외측 벽에 1 cm 가량의 열상이 있는 것을 확인하였다(Fig. 4A). 내시경적 역행성 담췌관 조영술을 종료한 후 천공에 대한 치료를 위하여 투명 캡을 상부위장관내시경 선단에 장착한 뒤 열상이 있는 부분에 접근하여 지혈클립(EZ-CLIP, standard type, 135°; Olympus Optical Co., Ltd.)으로 봉합하였다(Fig. 4B). 시술 후 1일째 복통 및 압통, 호흡곤란을 호소하여 단순 복부 방사선 및 복부 컴퓨터단층촬영을 시행하였으며, 후복강에서 대량의 유리 공기 및 종격동의 공기음영이 관찰되었다(Fig. 5). 임상경과가 악화되는 것으로 판단하여 외과 협진을 통한 수술적인 처치를 고려하였으나 생체징후가 안정적이며, 뇌경색 등 기저 질환이 있는 고령의 환자에서 수술 후 경과가 악화될 것으로 판단하여 보존적인 처치를 지속하기로 하였다.

Fluoroscopic image shows free retroperitoneal air.
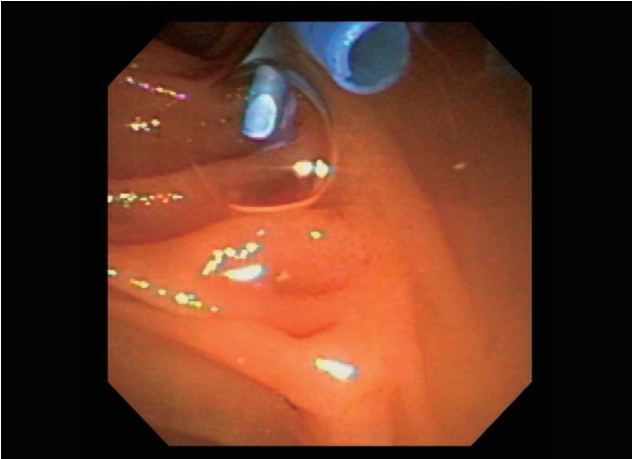
Image shows insertion of a plastic stent into the common bile duct.
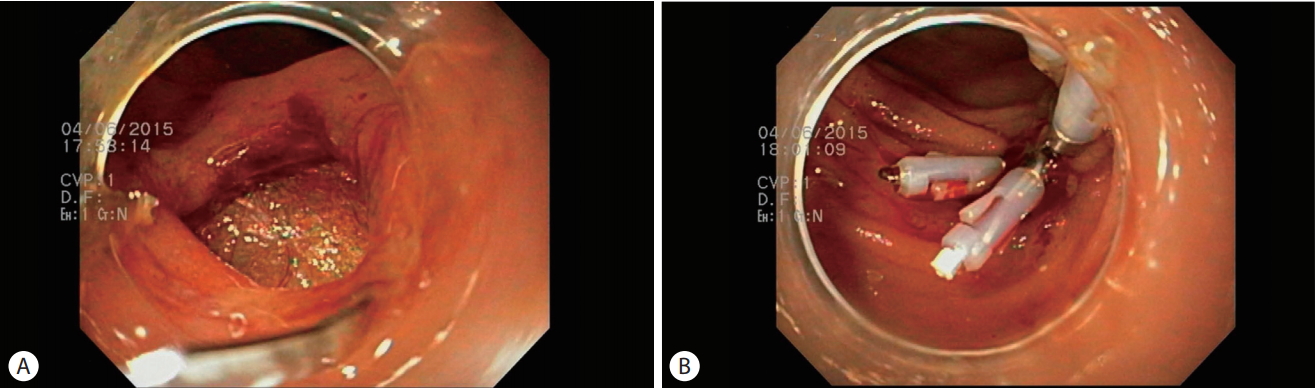
(A) Endoscopic image shows endoscopic retrograde cholangiopancreatography-related duodenal perforation. A hole measuring approximately 1 cm in diameter is observed in the lateral wall of the 2nd portion of the duodenum. (B) Multiple hemoclips have been used to achieve primary closure of the duodenal perforation.
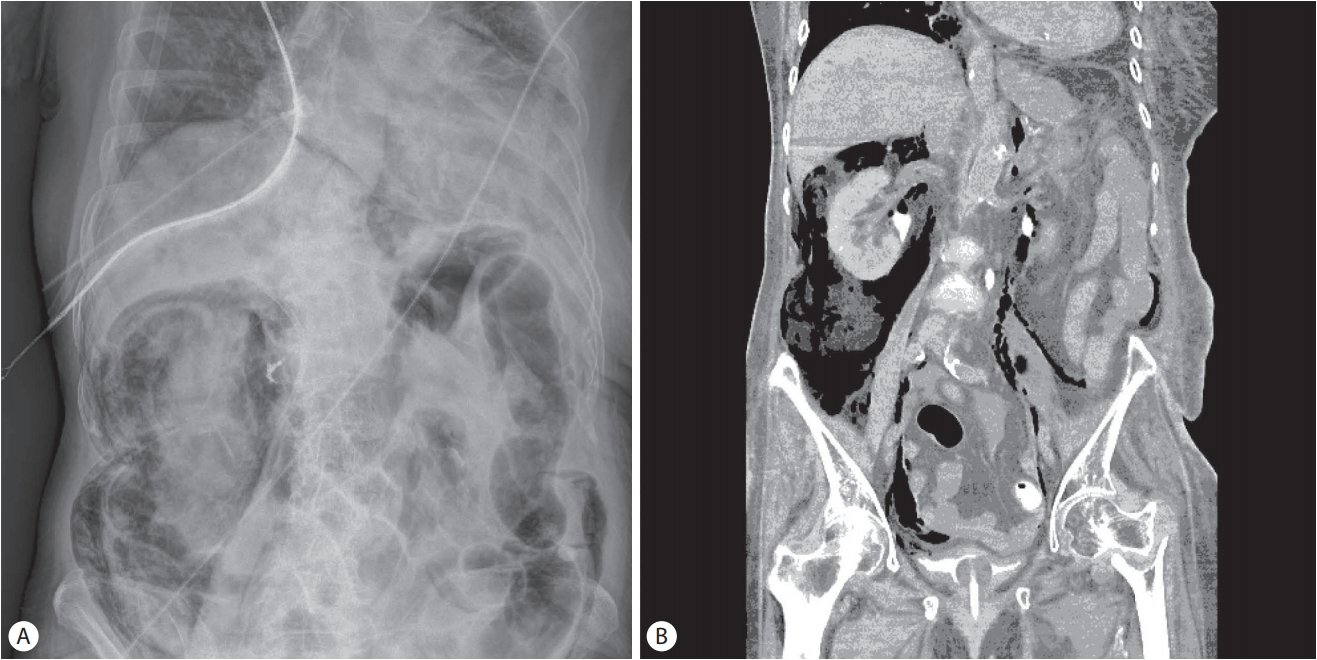
(A) Plain radiograph shows free retroperitoneal air after endoscopic retrograde cholangiopancreatography. (B) Enhanced abdominal computed tomography scan shows massive free retroperitoneal air.
환자는 중환자실에서 비위관을 유지하며 금식 및 비경구 영양공급, 광범위항생제, 산소를 공급하며 경과관찰하였고, 추적 검사로 시행한 단순 복부 방사선 검사에서 공기 음영은 점차 감소하였다. 시술 5일째 증상이 호전되어 경구 식이를 시작 후 시술 8일째 일반 병실로 전실하였다. 이후 담도암의 확진을 위한 내시경적 역행성 담췌관 조영술 등을 재시행할 것을 계획하였으나 고령의 환자로 추가적인 검사를 원하지 않아 퇴원하여 경과관찰하기로 하였다. 1개월간의 외래 통한 경과관찰 중 환자는 폐색전증의 재발로 타 병원에서 재입원하였으며 치료 중 패혈증으로 사망하였다.
2. Case 2
79세 여자가 내원 2주 전부터 시작된 황달, 가려움을 주소로 타 병원을 방문하였고, 복부 컴퓨터단층 촬영에서 담도암이 의심되어 검사를 위하여 내원하였다(Fig. 6). 과거력으로 50여 년 전 복막염으로 수술받았으며, 계통적 문진에서 피로 및 소화 불량을 호소하였으나 체중 감소는 보이지 않았다. 말초혈액 검사에서 백혈구 4,880/mm3, 혈색소 10.3 g/dL, 헤마토크리트 29.2%, 혈청 생화학 검사에서 아스파테이트아미노전이효소 39 IU/L, 알라닌아미노전이효소 39 IU/L, 알부민 3.2 g/dL, 총 빌리루빈 31.42 mg/dL, 직접 빌리루빈 25.40 mg/dL, 알칼리인산분해효소 249 IU/L, 감마글루타밀전이효소 102 IU/L, 탄수화물항원 19-9 >1,000 U/mL로 상승되어 있었으며, 이후 시행한 내시경 초음파 및 복부 자기공명영상에서 췌장 두부암의 담도 침범이 관찰되었다.
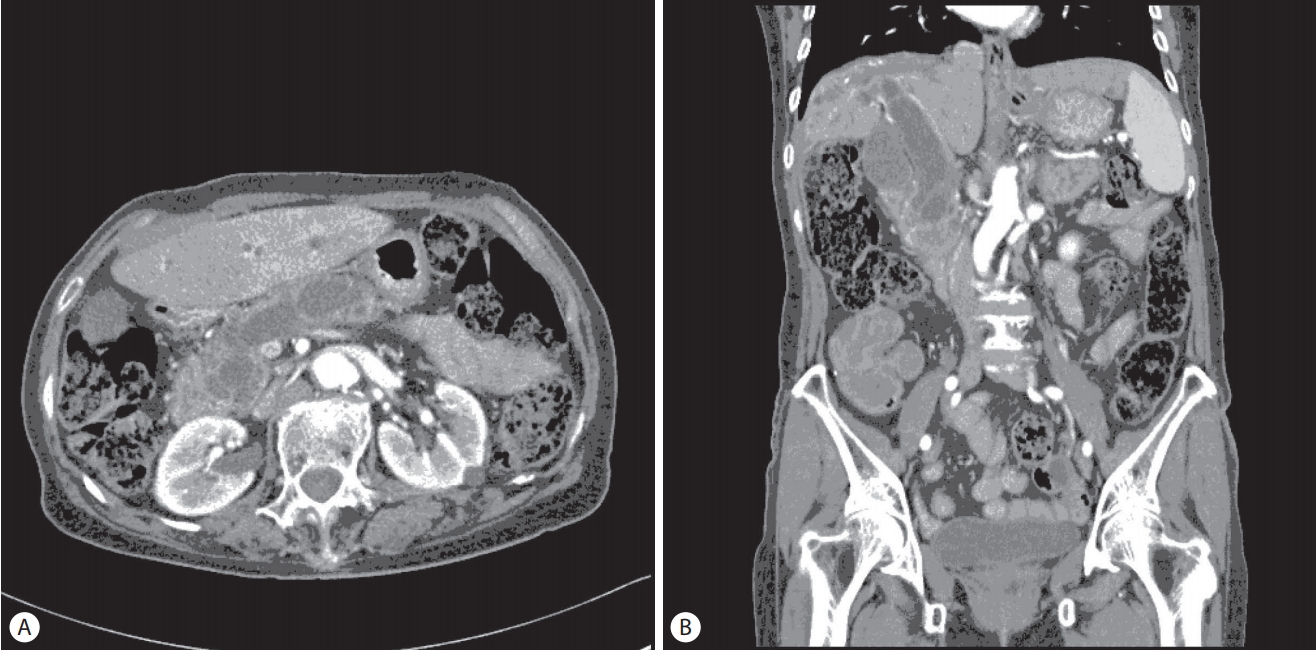
(A) Transverse computed tomography scan shows a mass-like lesion at the head of the pancreas. (B) Computed tomography scan (coronal view) shows mass-like conglomerates at the head of the pancreas associated with dilatation of the common bile duct and intrahepatic bile duct.
내원 1일째 담도 배액을 위하여 공기를 사용하여 내시경적 역행성 담췌관 조영술을 시행하였다. 십이지장경(TJF 240; Olympus Optical Co., Ltd.)을 이용하여 십이지장에 진입 중 십이지장 제2부에 출혈을 동반한 0.5 cm 크기의 열상이 발생하였고, 천공 가능성을 고려하여 상부 위장관 내시경(GIF-Q240; Olympus Optical Co., Ltd.)으로 변경하여 삽입 후 지혈클립(EZ-CLIP, standard type, 135°; Olympus Optical Co., Ltd.)으로 일차 봉합하였다(Fig. 7). 시술 직후 시행한 단순 복부 방사선 검사에서 봉합하였던 주변부로 유리 공기 음영이 보여 십이지장 천공으로 진단하였으며, 담도 배액을 위하여 경피적 담도 배액술 을 시행하였다. 이후 환자는 금식 및 비경구 영양공급, 광범위 항생제를 투여하였다.
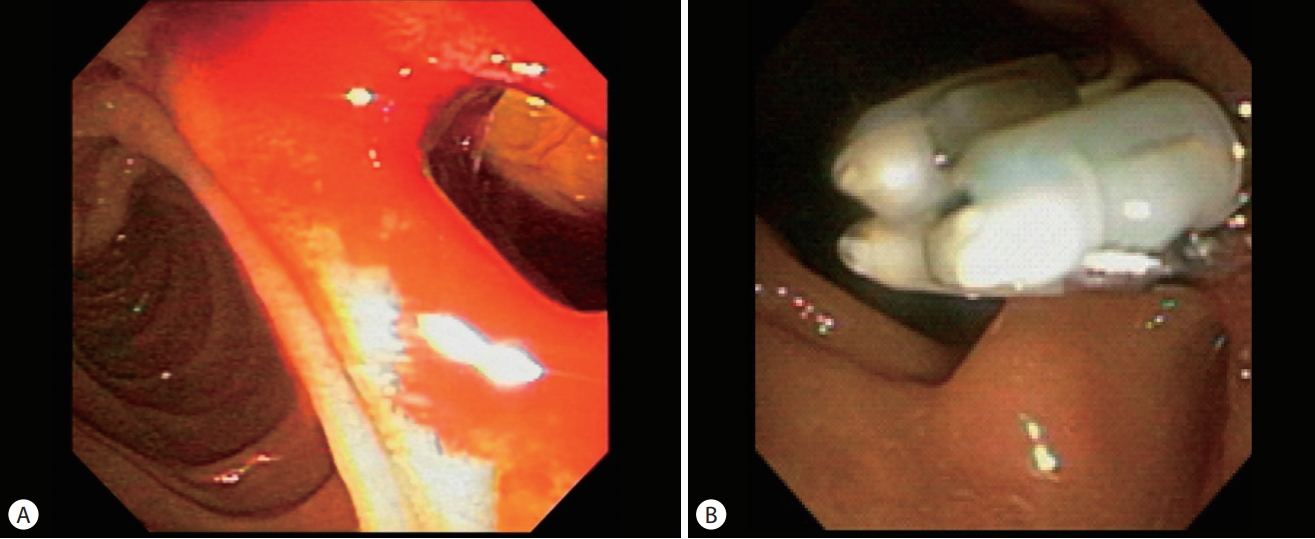
(A) Endoscopic image shows a hole in the lateral wall of the duodenal second portion measuring approximately 10 mm in diameter. (B) The duodenal perforation has been closed by using multiple hemoclips.
시술 2일째 38도 이상의 고열이 있었으나 C-반응단백 1.02 mg/dL로 경미한 상승이 있었으며 복막자극 등의 증상은 보이지 않았고, 시술 6일째부터 발열이 없으며, 증상 호전을 보여 식이를 허용하였다. 시술 11일째 다시 내시경적 역행성 담췌관 조영술을 시행하였으며 조직검사 를 시행하며 금속 담도 스텐트를 삽입하였다(Fig. 8). 이후 환자는 성공적 배액이 이루어져 시술 1개월 뒤 경피적 담도 배액관을 제거하고 퇴원할 수 있었다.
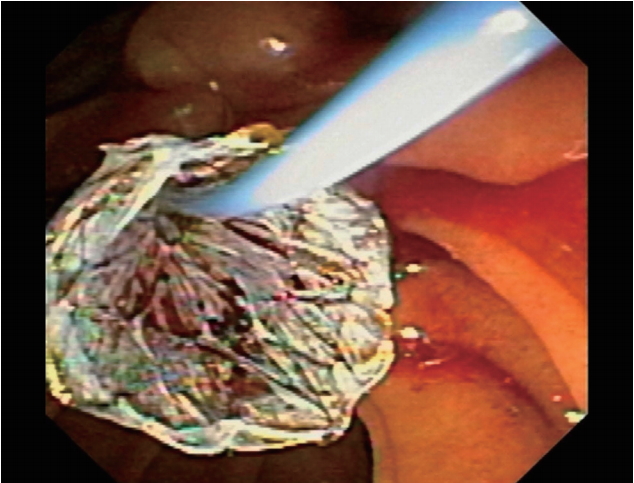
A fully covered self-expandable metal stent has been placed in the common bile duct after the primary closure of the duodenal perforation.
고 찰
췌담도 질환의 진단 및 치료에 있어 내시경적 역행성 담췌관 조영술은 중요한 수기이나, 시술과 연관되어 췌장염, 출혈, 담관염, 천공 등 중대한 합병증이 발생할 수 있다[3,4]. 특히 십이지장 천공은 치명적인 결과를 초래할 수 있는 합병증 중의 하나로 사망률이 10%까지 보고되고 있다[1,2].
시술 중 십이지장 천공이 발생할 경우, 복강내 지방조직 또는 타 장기를 확인하거나 조영제의 복강내 유출을 확인하여 즉각적으로 천공을 진단할 수 있다. 또한 시술 후 또는 검사 중 환자가 심한 복통이나 피부하 기종, 호흡 곤란을 보이는 경우 천공을 의심해볼 수 있다. 이러한 경우 시술 후 단순 복부촬영으로 복강내 유리가스 여부를 확인해 볼 수 있으며, 미세 천공이 발생한 경우에는 단순 복부 촬영만으로는 감별이 어려울 수 있어 복부 컴퓨터단층촬영을 시행하여 천공 확인에 도움을 받을 수 있다[5].
십이지장 천공이 발생하는 기전에는 여러 분류가 있으며, 이 중 Stapfer 등[6]은 해부학적 위치, 발생 기전, 중등도에 따라 천공에 대하여 분류하고 있다. 이에 따르면, 외벽 또는 내벽 천공일 경우를 제1형, 유두부 주위의 천공을 제2형, 원위부 담도 손상을 제3형, 후복강 공기만 관찰되는 경우를 제4형으로 분류하고 있다[6,7]. 이 중 제2형, 제3형인 경우 내시경 자체에 의하여 발생하는 제1형보다 천공의 크기가 작고 복강내 유출이 적어 환자가 안정된 상태일 경우 비수술적 치료를 권고하고 있다[8-10]. 일반적인 수술 적응증은 심각한 조영제 누출, 비수술적 치료 중 발생한 패혈증, 복막염, 경피적으로 배액되지 않는 복강내 액체 저류, 잔류하는 바스켓이나 담석이 있을 때, 환자의 상태가 악화될 때 등이다[11]. Polydorou 등[12]은 수술 적응증을 선별하기 위해서 4점 척도를 제시하였는데 천공 환자들을 비수술적으로 치료 중 발열, 빈맥, 복막 경직, 백혈구 증다증에 각각 1점을 부여하였을 때 3점 이상이면 수술을 시행하도록 제시하였다.
제1형 천공의 경우 전통적으로 수술을 권고하여 왔는데, 최근 들어 제1형 천공의 경우에 있어서도 endoclip이나 endoloop, fibrin glue와 endoclip을 이용한 치료 사례가 보고되고 있다[13-15]. 선행하는 연구들에서 공통적으로 내시경을 이용하여 천공을 봉합한 후 경비위관의 삽입, 금식, 항생제 치료 등의 보존적 치료를 통한 성공적인 치료 사례를 보고하였다. 따라서 만약 제1형 천공이 발생하더라도 즉각적으로 천공에 대한 봉합이 이루어지고, 환자의 상태에 따라 경비위관을 삽입 후 금식 및 조기 항생제 치료 등의 보존적 치료를 적절히 시행한다면 수술적 처치를 하지 않더라도 효과적인 회복을 기대해 볼 수 있을 것으로 생각된다.
Kaneko 등[3]은 비수술적 치료의 기준으로 국소적인 복막자극 증상과 더불어 적절한 크기의 천공 부위 및 모양 그리고 내시경 시야 확보가 가능한지 여부 등을 제시하였다. 저자들도 내시경을 이용하여 치료를 시도할 경우 천공 부위의 크기와 모양이 봉합하기에 적절한지, 내시경적인 시야가 충분히 확보될 수 있는지 고려해서, 클립을 이용한 봉합술이 부적절하게 이루어지거나 봉합술에 많이 시간이 지체됨으로 환자의 상태가 악화되지 않도록 주의해야 할 것으로 생각한다. 만약 즉각적인 천공의 치료가 어렵거나, 환자 상태가 불안정한 경우, 시술자가 미숙한 경우에는 치료의 적절성을 판단하여 수술적 치료를 고려해야 할 것이다.
본 증례의 경우, 시술 도중 천공이 조기에 발견되었고, 금식을 유지하고 있는 상태에서 시술이 이루어져 위와 십이지장에 있던 체액의 누출이 적고, 천공 부위가 상대적으로 크지 않았으며, 내시경으로 접근이 용이하여 클립을 이용한 적절한 봉합이 가능하였던 것으로 생각된다. 또한 2번째 증례의 경우 천공에 대한 처치 후 환자의 상태가 안정적으로 유지되어 시술 11일째 내시경적 역행성 담췌관 조영술을 재시행하여 금속 담도 스텐트를 삽입 후 체외 담도 배액관을 제거할 수 있었다. 그러나 아직까지 천공이 발생한 환자에게 있어 내시경적 역행성 담췌관 조영술을 재시행하는 것에 대한 지침 역시 없는 상태이다. 본 증례에 미루어, 환자의 경과가 안정적이라면 내시경적 역행성 담췌관 조영술을 재시행할 수 있을 것으로 생각되나 재천공이 되거나 다른 합병증이 발생한다면 환자의 경과에 치명적일 수 있기에 치료의 선택에 있어 주의가 필요할 것이다.
앞에서 살펴본 바와 같이 아직까지 내시경적 역행성 담췌관 조영술로 인한 제1형 천공이 발생하였을 때 수술적인 치료가 일차적인 치료로 권고되고 있다. 그러나 본 증례에서 살펴본 바와 같이 환자의 상태가 안정적이며, 내시경적인 봉합이 용이한 경우라면 선택된 소수의 환자에서 수술적 치료를 대체하여 조심스럽게 내시경적인 치료를 시도해 볼 수 있을 것이다.
Notes
Conflict of Interest
The authors have no conflicts to disclose.