경피경간담낭배액술과 관련된 흉강담도루의 내시경적 경유두담낭배액술을 통한 성공적 치료 증례
The Successful Treatment of Percutaneous Transhepatic Gallbladder Drainage Related Pleurobiliary Fistula via Endoscopic Transpapillary Gallbladder Drainage
Article information

Abstract
흉강담도루는 흔하지 않지만 가끔 경피경간담낭배액술 후에 발생할 수 있다. 본 증례는 경피경간담낭배액술 시행 후 발생한 흉강담도루로 진단받은 83세의 한국인 남성에 관련한 것으로, 경구용 담도경을 이용한 내시경적 경유두담낭배액술(SpyGlass DS system)을 통해 담낭 내 압력을 줄여 흉강으로 담즙의 유출을 줄일 수 있었다. 이후 환자는 호전되어 퇴원하였다.
Trans Abstract
The pleurobiliary fistula was not common but sometimes it could occur after percutaneous transhepatic gallbladder drainage. This report describes the case of an 83-year-old Korean male diagnosed with a pleurobiliary fistula after percutaneous transhepatic gallbladder drainage. The patient was treated with endoscopic transpapillary gallbladder drainage under the guidance of the peroral cholangioscopy with SpyGlass DS system. It can decompress pressure within the gallbladder. Leakage from the gallbladder into the pleura was reduced. Finally, his condition got better and he recovered.
서 론
흉강담도루(pleurobiliary fistula, thoracobiliary fistula), 담도흉강루(biliopleural fistula) 등 다양한 명칭으로 불리우는 흉강담도루는 담도계통과 흉강 사이의 연결이 형성되는 매우 드문 질환이다. 이에 대한 원인으로는 주로 복강과 흉강을 아우르는 외상, 간담도계의 악성종양, 선천기형 등 다양한 원인이 있지만 최근에는 간암에서의 고주파절제술 같은 시술과 관련되어 증례가 발생하고 있으며[1], 본 증례와 같이 경피경간담낭배액술(percutaneous transhepatic gallbladder drainage, PTGBD)에 의한 흉강담도루는 매우 드물게 보고되고 있다[2]. 흉강담도루의 국내 보고는 약 6건이며, PTGBD와 연관된 흉강담도루는 2건만이 보고되었다[3,4]. 치료는 담즙흉 치료를 위한 흉강배액관 삽입 및 항생제 사용, 그리고 담낭 내 압력 저하를 위한 PTGBD의 재실시가 주로 권고되고 있으며, 치료 반응이 좋지 않을 경우에 수술적 치료가 우선 고려되어야 한다[2,5]. 저자들은 흉강담도루과 담즙흉을 내시경적 경유두담낭배액술(endoscopic transpapillary gallbladder drainage, ETGBD)로 성공적으로 치료한 증례에 대한 경험을 공유하고자 한다.
증 례
83세 남자가 3일간의 경피경간담낭배액관 삽입 주위 통증을 주소로 응급실에 내원하였다. 환자는 기저 고혈압과 이상지질혈증 및 상행대동맥류가 있으며 내원 한 달 전 15 mm 크기의 담석 및 급성 담낭염 진단 하, 본원 외과에서 수술적 치료 대신 PTGBD를 통해 치료 후 호전되어 퇴원 및 추적관찰 중인 환자였다. 내원 당시 활력 징후는 혈압 118/71 mmHg, 분당 맥박수 107회/분, 호흡수 16회/분, 체온 37.4℃로 확인되었으며 내원 후 체온은 37.8℃까지 확인이 되었다. 신체검진상 우측 폐야에서 폐음이 감소되었고, 양측 폐하야에서 수포음이 확인되었으나, 복부 진찰 포함해서 다른 이상 소견은 없었다. 혈액 검사상 백혈구 5,870/mm3 (호중구 78.8%, 림프구 12.1%, 단핵구 6.6%), 혈색소 12.5 g/dL, 혈소판 232,000/µL, aspartate aminotransferase 21 IU/L, alanine aminotransferase 12 IU/L, total bilirubin 0.71 mg/dL, direct bilirubin 0.34 mg/dL, blood urea nitrogen 17.3 mg/dL, creatinine 1.19 mg/dL, C-reactive protein (CRP) 11.63 mg/dL 로 확인되었다 . 흉부 X-선과 전산화단층촬영에서우측 흉수 소견이 확인되었다(Fig. 1A). 복부 전산화단층촬영에서 담낭담석이 있으면서, 담낭벽의 비후나 담낭 주위 지방조직으로의 침윤 등은 관찰되지 않았다. 또한, 간농양성 병변이나 간내외담도확장 역시 관찰되지 않았다. 한편, 경피경간담낭배액관이 삽입된 복벽과 간장 사이에 저음영이 관찰되었다(Fig. 1B). 흉수에 대하여 진단적 흉강천자를 시행하였으며, 흉수는 장액성 색깔을 띄고 있었으며(Fig. 2), 흉수 결과는 삼출물로 백혈구 3,212/µL (다핵구 52.9%, 단핵구 47.1%), lactate dehydrogenase 811 U/L, glucose 113 mg/dL, Adenosine deaminase 53.7 IU/L, pH 7.406이었다. 감염 조절을 위해 10.2 Fr의 배액관을 우측 흉강 내로 삽입하였다 . 경피경관담낭배액관에서 흡인한 담균배양에서 extended-spectrum beta-lactamase (ESBL) positive Escherichia coli가 확인되었고 항생제 감수성 결과에 따라 항생제 meropenem을 사용하였다. 또한, 흉수배양에서 ESBL 음성 E. Coli가 동정되었다. 내원 당일에 경피경간담낭배액관이 기존 위치에서 이탈되면서(Fig. 3A), 흉강에서 담낭으로 조영제가 누출되는 것이 확인되어 담낭배액관을 재삽입하였다(Fig. 3B). 내시경역행담췌관조영술을 시행하여 담관 삽관 후, 담낭 내로 배액관 삽입을 시도하였으나, 계획대로 진행되지 못하였다. 경구담도경(Spyglass)의 도움으로 담낭관을 통해 담낭으로 가이드와이어(guidewire)를 위치시키고, 내시경적 ETGBD로 7 Fr, 10 cm 길이의 이중 돼지 꼬리 모양의 플라스틱 배액관 2개를 담낭 내에 삽입하였다(Fig. 4). 배액관 삽입 후에 우측 흉수는 빠르게 감소하여, 삽입 5일째 흉수배액관을 제거하였다. 이후로 흉수가 재발하지 않고 CRP가 3 mg/dL로 감소하고, 발열이나 복통 등 증상이 호전되어 7일만에 퇴원하였다.
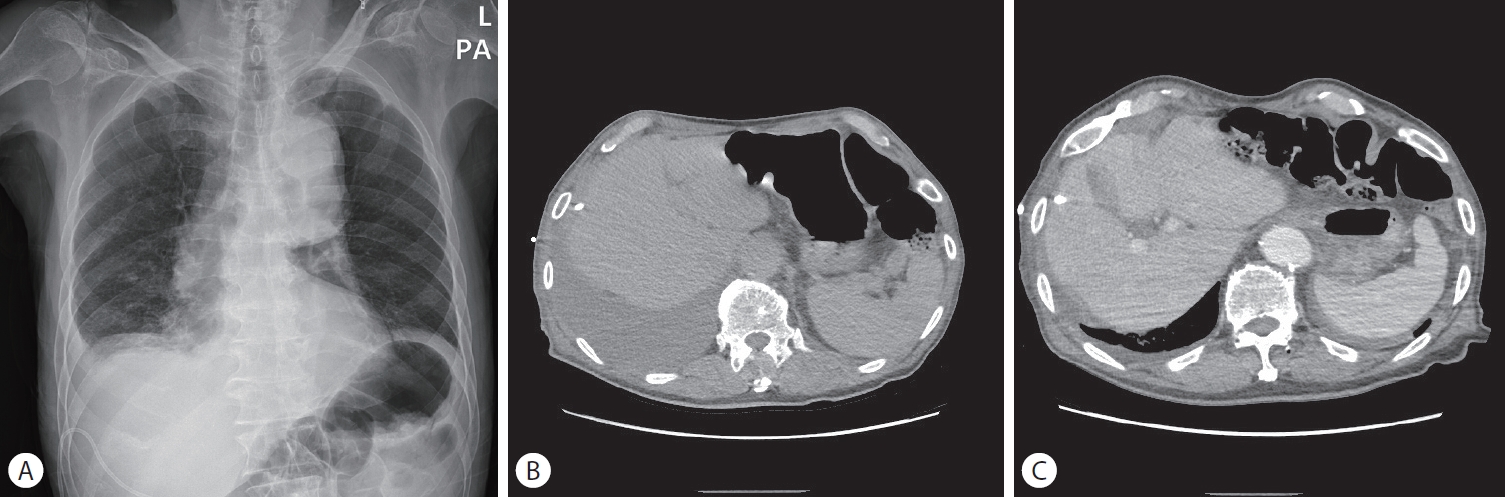
(A) Chest PA shows right costophrenic angle blunting implying right pleural effusion. (B) The chest CT shows right pleural effusion 38 days later after placing percutanous gallbladder drainage. (C) The chest CT shows more attached liver capsule with diaphragm when placing percutanous gallbladder drainage compared with B. PA, posterior anterior; CT, computed tomography.
The pleural fluid was serous at the initial diagnostic thoracentesis
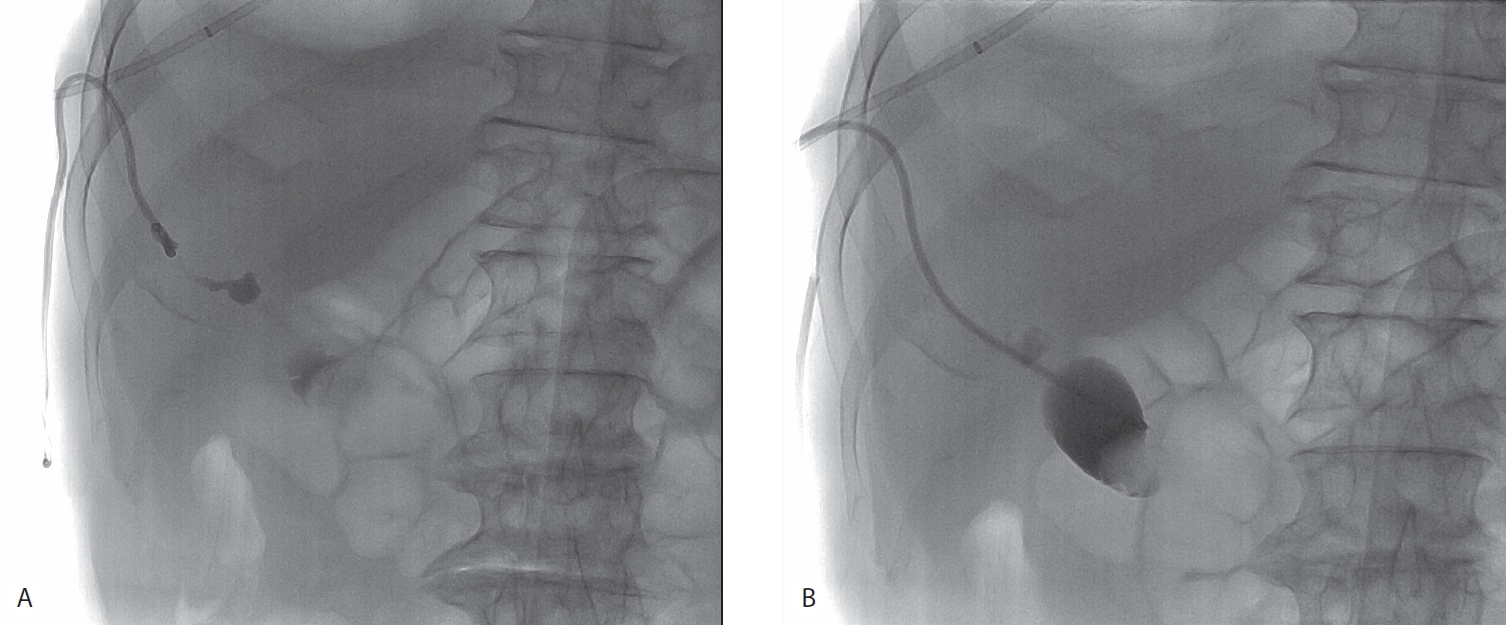
(A) The simple abdomen shows that the catheter was retracted with leakage of contrast to pleural space. (B) The cholecystogram shows that the catheter was repositioned and there was no more contrast leakage.
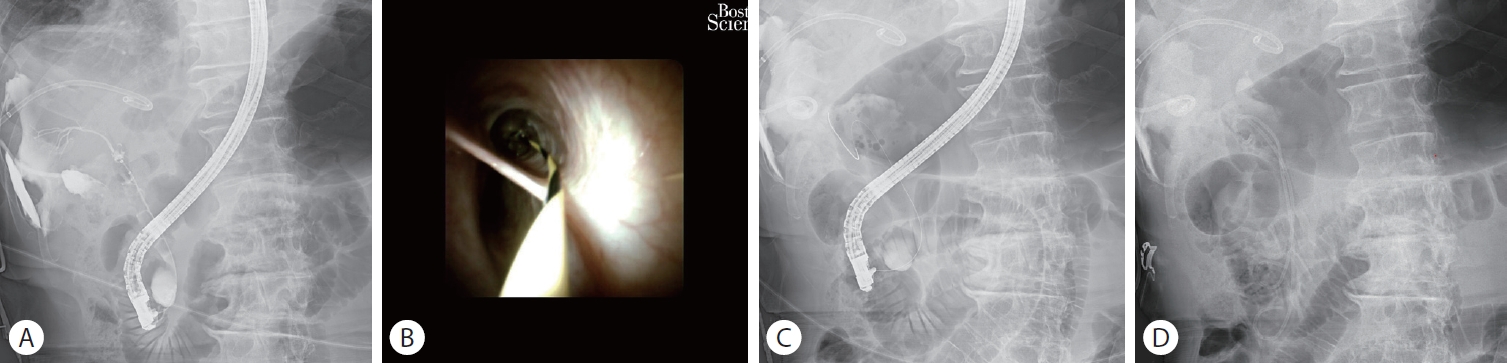
(A) The cholecystogram shows that there was the contrast leakage to pleural space. (B) The guidewire could be cannulated to the cystic duct under the peroral cholangioscopy with SpyGlass dS system. (C) There was the guidewire into the gall bladder. (d) The endoscopic transpapillary gallbladder drainage catheter was well placed.
고 찰
PTGBD로 인한 후기 합병증으로 흉강담도루는 극히 드물게 보고되고 있으며, 담즙성 흉막 감염이 균동정을 통해 확인된 경우는 국내에서 두 증례가 보고되었다[3,4]. 특히 본 증례에서는 이탈된 경피경관담낭배액관을 통한 조영술에서 담즙의 흉강으로의 유출을 직접 확인할 수 있었으며, 흉수와 담즙에서 같은 대장균이 동정되어 담즙성 흉막 감염을 동반한 흉강담도루로 진단하였다.
일반적인 흉강담도루의 치료는 대부분 흉수배액과 항생제를 사용하는 보존적 치료로 충분하며, 담낭 내 압력을 줄여서 흉강으로의 담즙의 유출을 줄이기 위해 PTGBD 및 내시경하 담도 내 스텐트 삽입술을 통해 간접적으로 담낭의 압력을 줄이는 치료가 권장되고 있다[2]. 흉강담도루의 치료로 본 증례처럼 ETGBD를 이용한 증례는 아직까지 보고된 바는 없다.
급성 담낭염의 초기 치료는 최근 업데이트된 도쿄가이드라인을 따르면, 복강경하 담낭절제술이지만, 환자들 중 고령이나 기저질환 등의 다양한 이유로 인해 수술이 어려운 경우에 PTGBD가 대체 치료로 활용되고 있다[6]. PTGBD가 매우 효과적이지만, 고령 및 기저질환으로 수술이 불가능한 경우에는, 결국 체외로 배액관을 장기간 유지해야 하는 경우가 많아서 환자들의 일상생활의 질이 떨어진다. 이런 이유로 내시경을 통한 담낭배액술을 시도하고 있지만, 담낭관을 통한 담낭으로의 삽관 성공률이 높지 않아서 보편적으로 시행되지는 못하고 있다. 문헌에 따르면 내시경역행담췌관조영술에서 담낭의 삽관 성공률은 70-80% 정도로 낮게 보고된다[7]. 최근에는 다양한 방법들이 시도되고 있는데, 초음파내시경 유도하 담낭배액술과 내시경적 ETGBD가 도쿄가이드라인에서도 숙련자에 한하여 PTGBD의 대체 치료로 제시되었다[6]. 또한 최근 담도경의 발달로 일본에서의 한 연구에 따르면 기존의 내시경역행담췌관조영술을 통한 내시경적 ETGBD보다 담도경을 이용한 내시경적 경유두담낭배액술(SpyGlass DS – assisted ETGBD)에서 담낭 삽관 성공률이 비약적으로 94%까지 높아진다고 제시하였다[8].
저자들은 본 증례에서 경피경간담낭조영술로 담즙이 흉강으로 유출되는, PTGBD 후 발생한 흉강담도루를 진단하고, 담낭 내 감압을 위해 담도경을 이용한 내시경적 경유두담낭배액술을 통해 배액관을 성공적으로 위치시켜, 빠른 기간내에 감염과 흉수를 조절할 수 있었다. 내시경적 ETGBD가 매우 효과적인 치료 방법임을 경험하여 이를 공유하는 바이다.
Notes
Conflict of Interest
The authors have no conflicts to disclose.