췌담도 질환에서 항생제의 올바른 사용
Practical Use of Antibiotics in Pancreatobiliary Diseases
Article information
Trans Abstract
Therapy with appropriate antimicrobial agents is an important component in the management of patients with liver, biliary and pancreatic infection. Acute cholangitis and cholecystitis are common conditions that may result in progressively severe infection. Infectious complications, both pancreatic (infected necrosis) and extrapancreatic (pneumonia, cholangitis, bacteremia, urinary tract infections, and so on), are a major cause of morbidity and mortality in patients with acute pancreatitis. Antimicrobial agents appropriate for initial therapy (empirical therapy or presumptive therapy) for various grades of severity of infections should be used. Local antimicrobial susceptibility patterns should be considered for use.
서 론
간담도계 감염에는 간, 담관, 담낭, 췌장과 비장에 관련된 감염들이 포함된다. 담도계 감염은 총담관이나 담낭에 흔히 발생하며 담즙 배설 경로의 폐쇄와 관련되어 있는 경우가 많다. 췌장조직 감염은 비감염성 급성 췌장염의 합병증으로 이차 감염이 되는 경우가 일차 감염되는 경우보다 더 빈번하다. 간농양은 화농성과 아메바성으로 나뉘는데, 특발성인 경우 외에도 급성 담도염이나 간, 담도계 종양, 복강 내 감염의 문맥을 통한 전파 등 다른 질환과 연관되어 발생할 수 있다. 이들 질환은 공통적으로 위장관의 세균총이 감염의 주 원인균으로 작용한다[1].
담관계에서 발생하는 세균 감염은 패혈증을 유발하거나 치명적일 수 있어 즉각적이고 적절한 치료가 필요하다. 특히 급성기의 담관계 감염은 항생제의 사용과 함께 조기에 내시경 혹은 경피경간 배액술을 시행하여야 한다. 급성 담낭염과 담관염이 의심되는 환자에서는 염증의 정도, 동반 질환의 유무, 의심되는 원인균에 대한 항생제의 항균력이나 감수성, 항생제의 담관계 침투 여부, 환자에 대한 과거 항생제 투여 병력 등을 고려하여 적절하게 항생제를 사용하여야 한다[2]. 무분별한 항생제 사용에 따른 내성균의 출현과 확산은 세균 감염증 치료에 항생제 처방을 도입한 후 지속적으로 문제가 되어 왔으며 다제 내성균 및 광범위 항생제에 대해 내성을 나타내는 균들의 출현은 감염증 관리에 대한 세계적인 위협으로 대두되고 있다.
본고에서는 국내[1] 및 일본[2], 미국[3] 등 세계 여러 나라에서 제시하고 있는 가이드라인을 검토하여 가장 적절하고 올바른 급성 담관염과 급성 담낭염의 진단과 경험적 항생제 요법, 급성 췌장염의 이차 감염과 항생제 요법에 대해 알아보고자 한다.
본 론
1. 담도계 질환(Antimicrobial therapy of biliary tract infection)
급성 담낭염/담관염(이하 담도계 염증)으로 대표되는 담도계 염증은 감염(infection)과 담도 폐쇄(obstruction)의 두 가지 요소가 복합적으로 작용하여 발생한다. 정상적으로 담즙은 무균 상태지만 담석, 수술 후 협착, 종양 등의 원인으로 인해 담도계에 완전 혹은 불완전한 폐쇄가 발생하면 여러 경로를 통해 감염이 발생한다. 담도계 질환의 감염 경로로는 십이지장으로부터의 상행 감염, 간으로부터의 하행 감염, 간동맥 및 문맥 등 혈관계를 통한 감염, 림프관을 통한 감염 등이 있다[4]. 담도계 염증으로 환자가 병원에 방문하면 문진 및 이학적 검사와 같은 초기 진단검사를 시행한 후 수술이나 응급 배액술의 적응증을 고려하면서 금식, 충분한 수액과 전해질의 보충, 진통제, 항생제를 투여한다. 특히 패혈성 쇼크가 의심되는 환자에서는 즉시 신속한 구호조치가 필요하다.
1) 진단(Appropriate Diagnostic Strategies)
급성 담도계 염증은 임상 증상, 검사실 소견, 영상 검사를 종합하여 진단하게 된다. 급성 담관염에서는 발열, 황달, 복통의 Charcot’s triad 소견이 나타나고, 급성 담낭염의 이학적 검사에서는 Murphy’s sign이 특징적이다[1]. 혈액검사에서는 말초혈 백혈구 증가, 적혈구 침강 속도 상승, C 반응성 단백 상승 및 혈청 빌리루빈, 알칼리성 인산분해효소, 감마글루타밀전환효소, 아스파르테이트 아미노전이요소, 알라닌 아미노전이요소 등의 간기능 수치가 상승한다. 영상 검사는 초음파, 전산화 단층 촬영, 간담도 주사검사 등이 있다[1]. 특히 급성 담낭염의 경우 초음파 검사는 담낭벽 비후, 담낭주위 체액 저류, 담낭 확장을 실시간으로 관찰할 수 있으며 검사 중에 초음파 탐촉자로 담낭을 압박하였을 때 통증이 유발되는 ultrasonographic Murphy’s sign이 92% 이상의 높은 양성예측도를 보여준다[5]. 따라서 미국 권고안에서는 담도계 염증이 의심되는 경우에 첫 번째로 시행하는 영상검사로 권고하고 있으며[3], 국내 진료지침에서도 일차적으로 권장한다[1]. 그러나 담도계 염증이 있는 많은 환자들이 먼저 응급실을 방문하고 있으며, 담석을 제외한 다른 담도폐쇄에 의해서도 염증이 발생하고, 다른 급성 복증과의 감별진단이 필요한 경우도 있어 초음파 검사만을 일차 검사로 하는 것이 타당한 지는 많은 검토가 필요하다고 생각된다.
2) 원인균
급성 담도계 염증에서 흔히 분리되는 균은 대부분 장내 세균총에서 기원한다. 호기성 균으로는 E. coli , K. pneumoniae, Enterobacter 같은 그람 음성균이 흔하다. 그람 양성균으로 장알균, 사슬알균이 흔하고 병원감염이나 ERCP나 수술력이 있는 경우에는 P. aeruginosa가 원인이 되기도 한다. 담관 수술력이 있거나 담관-장 문합이 있는 경우에는, 그렇지 않은 경우보다 Bacteroides, Fusobacterium, Clostridia 같은 혐기균이 더 자주 원인이 된다[2].
원인 균의 동정을 위해서는 미생물학적 검사인 혈액배양과 담즙배양을 시행한다. 배양 검사를 통하여 병원성 미생물을 진단할 뿐 아니라 중증도, 치료효과 판정과 합병증 발생시에 치료 방침의 결정에 있어 매우 중요한 역할을 한다. 국내 연구에서는 급성 담낭염의 담즙배양 양성률이 보고자에 따라서 또는 담석 유무에 따라 다양하지만[6,7], 원인균 규명에 도움이 되는 점을 고려하여 혈액배양과 채취 가능하다면 담즙배양을 권장한다[1]. 하지만 일부 후향적 연구에서는 모든 환자에게 시행하는 혈액 배양검사가 치료 방침과 결과에 큰 영향을 주지 못한다고 하여 무조건적인 혈액배양 검사는 권하지 않으며[8], 일본 권고안에서도 grade I 중증도 감염에서는 혈액배양 및 담즙배양을 무조건 권유하지는 않는다[2]. 또한 추적 담즙배양 검사에서 절반 이상이 진성 세균주가 아니라 는 연구도 있다[9]. 따라서 담도계 감염이 의심되는 환자가 방문하였을 때 가능한 혈액배양 및 담즙배양 검사를 시행하는 것이 좋겠지만 경증의 지역사회 발병 감염과 추적 담즙배양검사는 모든 환자에게 무조건적으로 시행하는 것은 지양할 필요가 있다.
3) 경험적 항생제 사용
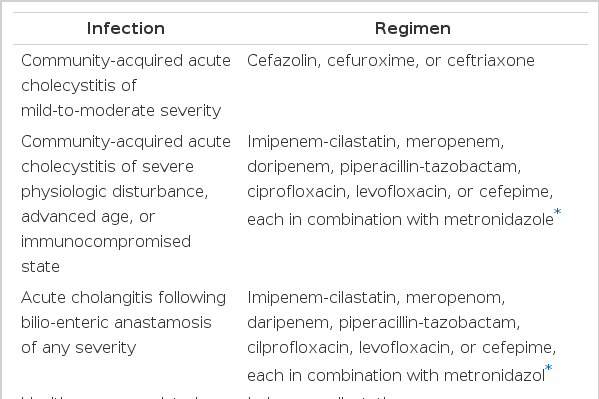
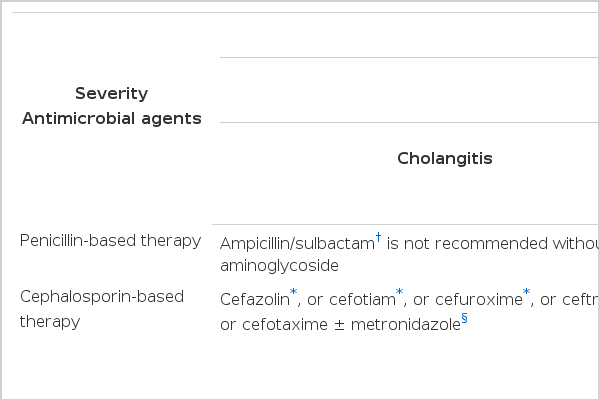
급성 담도계 염증 환자가 병원에 방문하였을 때 담석과 같이 폐색의 원인이 되는 병변을 제거하는 것과 함께 항생제를 투여하는 데 특히 패혈성 쇼크 환자에게는 가능한 빨리 투여하도록 한다. 미국의 권고안에서는[3] 1) 경증 또는 중등증의 지역사회획득 급성 담낭염이나 담관염에는 cefazolin, cefuroxime, ceftriaxone을, 2) 생리적 기능 이상이 중하거나, 고령이거나 면역저하 상태인 경우, 증상 중증도에 관계없이 담관-장 문합 후 발생한 급성 담관염에서는 혐기균에 대한 항균효과를 포함하는 imipenem/cilastatin, meropenem, doripenem, piperacillin/tazobactam, ciprofloxacin+metronidazole, levofloxacin+metronidazole, cefepime+metronidazole을, 3) 증상 중증도에 관계없이 의료관련 담관 감염에는 2)의 항생제에 더하여 vancomycin 추가를 권장하고 있다(Table 1). 의료관련 감염(health care-associated infection)은 지역사회발병(community-onset)과 병원발병(hospital-onset) 감염을 모두 포함하는데, 지역사회발병 의료관련감염은 다음 의료 위험인자-1) 입원 당시 침습적 장치가 있는 경우, 2) MRSA 감염이나 집락의 병력이 있는 경우, 3) 배양일 이전 12개월 이내에 수술, 입원, 투석, 또는 장기요양시설 거주력이 있는 경우-중 적어도 한 가지 해당 사항이 있어야 한다. 병원감염은 병원 입원 48시간 후에 감염되었고 정상적으로는 무균상태인 부위에서 균이 검출된 경우를 말한다. 의료관련 감염과 중증의 감염에서는 녹농균과 혐기균에 대한 항균력이 있는 항생제가 포함되어야 한다. 일본의 권고안도 미국의 지침과 큰 차이를 보이지 않으며 그 내용은 표와 같다(Table2)[2]. 국내에서는 1세대 cephalosporin에 대한 E. coli나 K. pneumonia의 내성률이 50% 가까운 국내 항생제 내성 현황을 고려하여[10], 급성 담낭염이나 담관염의 흔한 원인균인 장내 그람음성균에 대해 1세대 cephalosporin을 사용하는 것은 적합하지 않다고 하였고, 다음과 같이 권고하였다[1]. 경증 또는 중등증 급성 담관염/담낭염 환자에서 항혐기균 항생제를권장하지 않는다. 경증 또는 중등증 급성 담관염/담낭염 환자에서 다음의 항생제를 권장한다: cefuroxime, ceftriaxone, levofloxacin, ciprofloxacin. 중증 급성 담관염/담낭염 환자, 중증도에 관계없이 담관-장 문합(biliary-enteric anastomosis)을 한 환자, 중증도에 관계없이 의료관련 급성 담관염/담낭염 환자에서 다음의 항생제를 권장한다: ceftazidime 또는 cefepime과 metronidazole 병합, cefoperazone/sulbactam, piperacillin/tazobactam, meropenem, imipenem/cilastatin. 그러나 항생제를 사용하는데 있어 항상 고려해야 할 점은 그 지역의 항생제 감수성 형태가 어떤 지를 생각하고 처방하는 것이 중요하다는 것이다.
내시경 역행성 담췌관 조영술 검사 전에 예방적 항생제 사용에 대하여 최근 2개의 메타 분석이 있었다. Bai 등은 예방적 항생제 사용이 담도염을 줄여주지 못했다는 반면 코크란메타 분석에서는 예방적 항생제 사용이 전체적인 사망률을 줄여주지는 못했지만 균혈증, 담도염, 췌장염의 발생은 줄여주는 것으로 보고하였다[11,12]. 대한췌담도학회 총담관결석 진료 지침에서도 담도폐쇄나 패혈증의 양상을 보였던 환자 혹은 면역 억제환자에서는 예방적 항생제 사용을 권장하고 있어 이러한 환자에서는 검사 전에 예방적 항생제를 사용하는 것이 좋겠다[13].
4) 사용기간(Table 3)
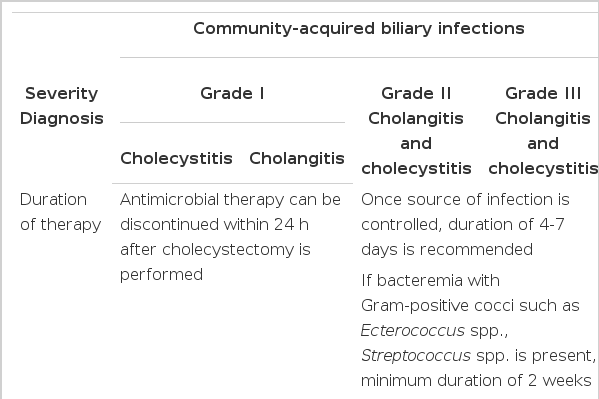
지역사회획득과 의료관련 감염 급성 담낭염이나 담관염에서 적절한 항생제 사용 기간에 대한 무작위 비교연구는 아직까지 없다. 하지만 현재까지 발표된 권고안 및 전문가 의견을 종합하면 담낭염에서 담낭 절제술 후 24시간까지만 사용할 것을 권장한다[2]. 담낭 절제술 동안에 담낭의 괴사, 천공, 기종이 있는 경우에는 4~7일간의 항생제 사용이 권장된다. 담도염에서는 폐색 등의 원인병소 조절이 적절히 이루어진 후 4-7일 동안 항생제 사용을 권장하며, 잔류 담석이 있거나 담도 폐쇄가 남아있는 경우에는 폐쇄가 해결될 때까지 항생제 사용을 지속하도록 한다. 장알균, 사슬알균 같은 그람 양성균에 의한 균혈증인 경우에는 최소 2주간의 항생제 사용을 권고하고 있다[2].
5) 항생제 교체
경구식이가 가능한 환자는 경구용 항생제로 바꾸어 치료를 할 수 있다. 다만 감염이 충분히 조절된다면 원인균의 항생제 감수성을 고려하여 fluoroquinolones (ciprofloxacin, levofloxacin, or moxifloxacin), amoxicillin/clavulanic acid, 또는 cephalosporins 등의 경구용 항생제를 선택할 수 있다[2].
2. 췌장질환(Antimicrobial therapy of pancreatic infection)
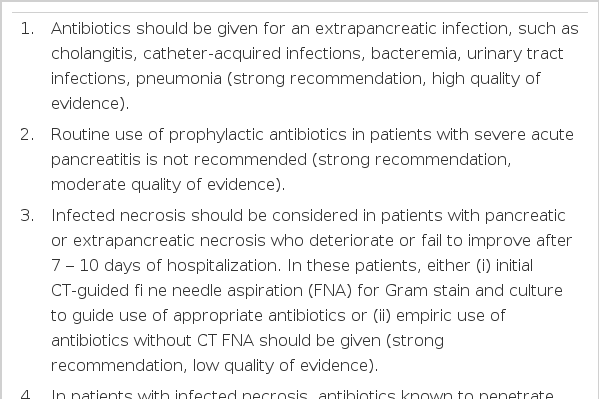
급성 췌장염의 80% 정도는 경한 임상경과를 보이지만, 약 20%는 췌장조직 괴사 및 전신적인 합병증을 나타내는 위중한 경과를 밟게 된다. 급성 췌장염에서 항생제 투여가 필요한 감염성 합병증은 폐렴, 담도염, 균혈증, 요로감염과 같은 췌장 외 감염증과 감염성 괴사와 같은 췌장의 감염으로 크게 나눌 수 있다. 대부분 원내감염이며 급성 췌장염 환자의 사망률을 높이는 주요한 요인이다[14]. 따라서 감염이 의심되는 급성 췌장염 환자는 감염의 원인을 찾는 중에도 바로 항생제 치료를 시작해야 한다. 급성 췌장염의 초기에도 발열은 발생할 수 있으므로 배양검사에서 음성이고 감염의 원인이 밝혀 지지 않는 경우에는 항생제 치료를 중단하여야 한다. 2013년 발표된 미국 급성 췌장염의 치료 가이드라인은 표와 같다(Table 4)[15].
1) 예방적 항생제
Santorini Consensus Conference에서는 모든 중증 급성 췌장염에서 예방적 항생제 투여를 강력히 권장하였으나[16], 최근 메타 분석에 의하면 중증 췌장염에서 예방적 항생제 사용의 이득이 없어 임상적으로 또는 배양결과 양성으로 감염이 진단되기 이전에는 예방적 항생제 투여를 권장하지 않는다[15].
췌장의 괴사가 지속되면 감염의 위험성과 염증 반응이 증가할 수 있다는 근거 하에 과거에는 개복 수술로 괴사된 부위를 제거하는 방법이 표준적 치료법이었다. 그러나 이 후 연구들을 근거로 무균성 췌장 괴사를 가진 환자에서 췌장염 발생 2-3주 내에는 외과적 제거보다는 내과적 치료가 표준치료로 자리잡았다[17]. 무균성 췌장괴사와 비교하여 볼 때 세균성 췌장괴사는 사망률이 매우 높기 때문에(mean 30 %, range 14-69%) 예방적 항생제 투여를 권장하였으나 최근 연구들은 예방적 항생제 투여의 이득을 보여주지 못했다[18]. Cochrane review에 의하면 예방적 항생제 투여는 사망을 감소시키지만(투여군 6%, 대조군 15.3%, odds ratio 0.37, 95% 신뢰구간 0.17, 0.83), 괴사조직의 감염률에는 영향이 없고 (투여군 20%, 대조군 27.8%, odds ratio 0.62, 95% 신뢰구간 0.35, 1.09), 진균감염의 위험률을 증가시키지도 않았다(투여군 4%, 대조군 4.9%, odds ratio 0.83, 95% 신뢰구간 0.30, 2.27)[18]. 따라서 무균성 췌장괴사에 있어 예방적 항생제 사용을 권고하지 않는다.
항생제 선택에 있어 췌장 조직에 잘 침투하는 약제를 선택하는 것이 바람직하며, 대부분의 원인균에 대해 최소억제농도(minimum inhibitory concentration; MIC)에 도달하는 항생제로는 carbapenems, quinolones, metronidazole, highdose cephalosporins이 있다[15,19]. 항진균제는 Candida 감염이 증명되면 사용하고 예방적 사용은 추천하지 않는다[15].
2) 감염성 궤사
감염성 췌장 괴사의 치료는 괴사된 췌장이나 췌장 주위 조직을 제거하는 것이 기본적인 치료법이고, 과거에는 주로 개복을 통한 조기 수술이 시행되었다. 수술적 괴사 제거술이 그 동안 권장된 이유는 감염된 괴사 조직을 제거할 수 있고, 괴사된 조직 내로 잘 침투되는 항생제가 없었으며, 대부분의 환자들이 조기에 처치가 필요한 불안정한 상태였기 때문이었다. 하지만 조기수술에 대한 효과에 대한 의문이 제기되면서 지연 수술과 조기 수술을 비교하는 보고들이 발표되었다[20,21]. 대한 췌담도학회 급성 췌장염 진료지침에서도 괴사성 췌장염에서 수술적 치료는 췌장염 발생 4주 후로 최대한 연기하여야 하며 환자의 상태가 안정된 감염성 췌장 괴사의 경우에는 항생제 치료와 보존적 치료를 하면서 추적 관찰할 수 있다고 권고하고 있다[22]. 따라서 이 기간에 적절한 항생제 사용이 중요하다.
결 론
담관계에서 발생하는 세균 감염은 패혈증을 유발하거나 치명적일 수 있어 즉각적이고 적절한 치료가 필요하다. 특히 급성기의 담관계 감염은 필요에 따라 적절한 배액과 함께 항균제 치료가 중요하다. 급성 담낭염과 담관염이 의심되는 환자에서는 염증의 정도, 동반 질환의 유무, 의심되는 원인균에 대한 항균제의 항균력이나 감수성, 항균제의 담관계 침투 여부, 환자에 대한 과거 항균제 투여 병력 등을 고려하여 적절하게 항균제를 사용하여야 한다[2].
또한 췌장염의 치료에서도 불필요한 예방적 항생제 사용은 권고하지 않으며, 발생한 췌장괴사의 치료는 수술적 치료를 조기에 시행하기 보다는 감염된 부위를 배액하는 경피적 또는 내시경 중재술을 시행하여 염증과 감염을 최소화하고, 필요하면 다음 단계로 복강경이나 내시경을 이용한 최소침습 괴사 제거술 또는 수술적 괴사 제거술을 추가적으로 시행하는 단계적 접근법으로 발전하고 있어 환자에게 적절한 항생제를 투여하는 것이 매우 중요하겠다.
Notes
The author has no conflicts to disclose.