내시경유두괄약근절개술 후 출혈의 내시경 치료
Post-Endoscopic Sphincterotomy Bleeding: Strategic Approach with Multiple Endoscopic Arms
Article information
Abstract
내시경역행담췌관조영술(ERCP)은 췌담도 질환의 진단과 치료에 필수적인 시술이며, 내시경유두괄약근절개술(EST)은 ERCP를 성공하기 위한 관문이다. EST를 시행하기 위한 장비의 발전에도 불구하고, EST 후 발생한 출혈은 여전히 치명적인 합병증으로 남아있다. EST 직후에 발생한 출혈은 내시경 시야를 방해하여 성공적인 ERCP를 마칠 수 없게 하며, EST 후 지연형 출혈의 경우에는 혈담즙과 이에 의한 담도염, 심지어 혈역학적 쇼크까지 유발할 수 있으므로 주의가 필요하다. 다행히도 대부분의 출혈은 자발적으로 멈추지만, 임상적으로 의미 있는 출혈량이 있거나, 지속적인 출혈에서는 1차적으로 내시경 지혈술이 필요하다. 에피네프린을 혼합한 식염수의 주사, 전기응고법, 클립이나 밴드를 이용한 기계적 지혈법까지 다양한 내시경적 지혈법이 있으며, 이러한 방법은 대부분 위장관 출혈의 지혈술에서 사용되는 방법을 가져온 것이다. ERCP를 시행하는 의사는 다양한 내시경적 지혈술을 모두 숙지하고 있어야, 한가지 지혈술로 실패한 경우에 다른 방법의 지혈술로 전환을 할 수 있어야한다. 또한 내시경적 지혈술에 실패한 경우에는 혈관조영술이나 수술로 출혈을 치료할 수 있는 결정을 할 수 있어야만 한다.
Trans Abstract
Endoscopic retrograde cholangiopancreatography (ERCP) is an essential method for diagnosis and treatment of various pancreatobiliary diseases and endoscopic sphincterotomy (EST) is the gateway to complete ERCP. Although techniques and instruments for EST have improved, bleeding is still the most common complication. Treatment of immediate post-EST bleeding is important because blood can interfere with subsequent procedures. Additionally, endoscopists should be cautious about delayed bleeding may cause hemobilia, cholangitis, and hemodynamic shock. Most cases of post-EST bleedings will stop spontaneously, however, endoscopic management is necessary in case of clinically significant and persistent bleeding. Various endoscopic methods including epinephrine or fibrin glue injection, electrocoagulation, hemoclipping and band ligation et al can be used through a side-viewing or forward-viewing endoscope similar to those used in hemostasis of peptic ulcer bleeding. Endoscopists who perform ERCP should use various methods of endoscopic hemostasis strategically.
서 론
내시경유두괄약근절개술(endoscopic sphincterotomy, EST)은 내시경역행담췌관조영술(endoscopic retrograde cholangiopancreatography, ERCP)로 담췌관 질환을 진단하고 치료하기 위한 필수적인 관문이다. 하지만 췌장염, 출혈, 담관염, 장천공 등의 합병증이 발생할 수 있어 항상 주의가 필요하다. 전체적인 시술 합병증 발생률은 4-10% 정도이며, 치명적인 경우는 0.5% 미만으로 알려져 있다[1]. EST 후 발생한 출혈(post-EST bleeding)은 정의를 어떻게 하느냐에 따라 1-48%의 다양한 발생률을 보인다[2]. 출혈은 그 자체도 무서운 합병증이지만, 지혈술 과정에서 췌장염 또는 천공 등의 추가적인 합병증을 유발할 수 있으므로 더욱 주의가 필요하다. 이에 본고에서는 post-EST 출혈의 내시경적 지혈을 중심으로 다루려고 한다.
본 론
1. Post-EST 출혈의 분류와 역학
Post-EST 출혈의 대부분은 약간의 울혈성 출혈이며 다행히도 대부분 저절로 멎기 때문에 임상적으로 큰 어려움을 유발하지는 않는다[3]. 그러나 동맥성이나 대량출혈이 간혹 발생하게 되면 내시경 시야를 가리게 되므로, 지혈술에도 곤란을 겪으며 ERCP 시술의 목적을 달성하지도 못하게 된다. 시술 후 출혈의 정도는 Cotton 등[4]의 제시한 다음과 같은 분류가 주로 사용되고 있다. 경증(mild)은 혈중 헤모글로빈이 3 g/dL 미만으로 떨어지고 수혈이 필요 없는 경우이고, 중등증(moderate)은 4 유닛 이하의 수혈이 필요하지만 혈관조영술이나 수술이 필요하지 않은 경우이며, 증증(severe)은 5 유닛 이상의 수혈이 필요하거나 중재적 치료(혈관조영술이나 수술)가 필요한 경우이다(Table 1)[4]. 출혈이 발생한 시기에 따라 분류할 수도 있는데, 출혈이 발생한 시기에 따라 시술 중 발생한 즉각(immediate) 또는 조기(early) 출혈과 시술 후 수 시간 또는 수일이 지나 발생하는 지연(delayed) 출혈로 분류된다[2,4,5]. 과거에는 혈색소 감소가 동반될 정도의 출혈이 2-5% 빈도로 보고되었지만, 최근의 연구에서는 1-2% 감소된 빈도로 보고하고 있다[6-8]. 이러한 원인은 명확히 제시되고 있지는 않지만, papillotome을 비롯한 ERCP 부속기구의 발전과 출혈위험군에 대한 사전 조치 등이 가능한 원인으로 고려될 수 있다.

2. 출혈의 위험인자
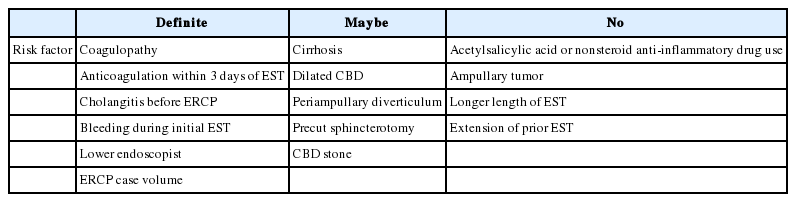
Post-EST 출혈의 위험인자로는 환자측 인자, 해부학적 인자, 기술적 인자로 분류할 수 있다. Freeman 등[5]은 여러 연구 결과에 따라 위험인자 분류를 크게 확정적(definite; 대부분의 연구들의 다변량 분석에서 의미를 가짐), 가능성 있는(maybe; 여러 연구들의 단변량 분석에서 의미) 그리고 관련 없음(no; 의미 있는 결과를 보인 연구 결과가 없었던 경우) 세 가지로 분류하였다(Table 2). 확정적 인자들에는 출혈경향이 있는 환자, 3일 이내에 항응고제 사용, 시술 전 담관염, EST 도중 출혈, 시술 의사의 경험이 적은 경우를 제시하였고, 가능성있는 인자들로는 간경변, 확장된 총담관, 유두부 주위의 게실, 예비괄약근 절개술, 담도담석이 있는 경우이며, 아스피린과 비스테로이드성 소염제의 사용, 유두부 종양, 괄약근 절개 길이나 추가적인 절개술은 출혈에 영향을 주지 않았다.
상기의 위험인자들 중 환자 측 또는 해부학적인 위험인자가 있는 경우에는 ERCP의 경험이 충분한 시술자가 시행하여 기술적인 측면에서의 위험을 줄이는 것이 의미가 있을 것이다. 또한 혈소판 수가 낮거나, 간경변 등의 이유로 프로트롬빈 시간이 증가된 환자는 혈소판 수혈이나 신선동결혈장 및 비타민 K를 투여하는 준비가 필요하다. 혈액응고장애가 의심되는 담관결석 환자에서는 EST와 비교하여 출혈의 발생이 적다고 알려진 유두부 풍선확장술을 고려할 수 있다[9-11]. 항응고제 사용에 따른 준비는 미국소화기내시경학회(American Society of Gastrointestinal Endoscopy)의 가이드라인을 따르는 것을 권고한다[12].
3. 내시경 지혈술의 종류와 방법
내시경적 지혈술에는 주사침을 이용한 주입법, 열응고술을 이용한 방법, 압박이나 클립 등을 이용한 기계적 방법이 있다. 상황에 따라 내시경 치료법의 선택은 다를 수 있으며, 순차적으로 이용될 수 있다. 그리고 내시경 치료에 실패한 경우에 혈관조영술을 이용한 색전술과 수술도 고려할 수 있다.
1) 주사침을 이용한 주입법(injection therapy)
희석된 에피네프린을 절개한 부위와 그 주변에 주사침을 이용하여 주입하는 지혈술이 가장 많이 사용되어 왔다. 에피네프린은 1:10,000으로 희석하여 주입하며, 치료 효과에 대하여 96-100%로 보고되기도 하였다[6]. 주의해야 할 점으로는 첫째, 측시경의 특성으로 주사침이 내시경 선단 부위를 통과하며 피막을 뚫고 내시경 채널을 손상할 수 있으므로 주의가 필요하며, 둘째, 에피네프린의 전신 흡수에 따른 심장 발작의 가능성을 유의하여야 한다[13].
최근 에피네프린 주입으로 지혈이 실패한 경우에 피브린 글루(fibrin glue)를 주입하여 지혈에 성공한 보고들이 있다[14,15]. 가능한 지혈법이기는 하지만 EST 후 발생한 출혈에 있어서는 췌관의 입구를 막아 췌장염이 발생할 수 있으므로 췌장염을 예방하기 위하여 미리 췌관에 스텐트가 삽입되어 있다면 고려해 볼 수 있다.
2) 열 응고법(thermal coagulation)
출혈하는 혈관에 열을 가하여 조직의 부종과 단백질 변성, 혈관 수축 등에 의하여 지혈을 일으키는 열응고법에는 전기나 빛 에너지를 이용하여 간접적으로 열을 발생시키는 전기응고법, 아르곤 플라즈마 응고법 및 레이저 응고법 등이 있다[16]. 이러한 열 응고법을 post-EST 출혈의 지혈에도 사용해왔다[17,18]. EST에 사용한 표준형 절개도를 그대로 사용하여 응고파를 내보내어 지혈에 사용할 수도 있지만, 다량의 출혈에는 효과적이지 않다. 열 응고법에 사용되는 기구(devices)는 대부분 상부 위장관 내시경 지혈술에 사용하는 것과 같다. 크게 도자(probe)형과 겸자(forcep)형이 있으며, 여러 제조사에서 공급하고 있다. 도자형은 출혈 부위에 전극을 접속하고 열을 가하는 방식으로 용종절제술용 올가미(polypectomy snare)를 대용으로 사용하기도 한다. 간편하게 사용하기 좋다는 장점이 있지만, 열이 전달되는 깊이와 범위가 환자의 장움직임이나 호흡에 따라 크게 변할 수 있고, 출혈되는 혈관을 더 깊게 파고 들어가서 더 큰 출혈을 일으킬 수 있으므로 응고파를 보내는 시간을 짧게 유지해야 하고 시술자의 숙련이 필요하다. 겸자형의 경우 출혈되는 혈관을 잡고 응고파를 내보내므로 정확하고 한정된 부위로만 열이 가해지는 장점이 있지만, ERCP에 사용되는 측시경의 구조적 특성으로 인하여 보이는 화면의 상방(해부학적으로 근위부)의 출혈 부위에 접근이 어렵고, 조준 또한 쉽지 않다. 이러한 어려움은 아르곤 플라즈마 응고법을 사용할 때도 마찬가지이다[19,20]. 출혈 부위의 해부학적 위치와 확보되는 시야에 따라 두 가지 형태의 기구를 적절히 사용할 수 있다면 더 좋은 치료 결과를 낼 것이다. 열 응고법을 사용하기 전에 주사침을 이용한 주입법으로 지혈을 유도하거나, 대량 출혈의 경우에 시야를 확보하는데 도움을 받을 수 있다. 십이지장경으로 접근이 어려운 경우 직시경으로 바꾸거나 직시경 선단부에 캡(cap)을 씌어 접근을 시도하면 도움이 될 수 있다[21-23]. 특히, 유두부 주위의 게실이 있거나 주변에 유착이 있는 경우 등에서 직시경으로 유두부에 접근을 하면 확연히 좋은 시야를 얻는 경우가 있으므로 측시경으로 계속 지혈에 실패하는 경우 직시경으로 바꿔볼 수 있다.
3) 기계적 지혈(mechanical hemostasis)
기계적인 지혈법으로 시술 중 발생한 출혈에 대하여 풍선을 이용한 압박이 도움이 될 수 있다는 과거 고찰에서 설명이 있고, 임상에서도 많은 시술의들이 담석제거용 풍선을 이용하여 출혈이 있는 유두부에 압박을 하는 지혈법을 사용하고 있다[24]. 하지만, 이에 대한 효과를 전향적으로 연구한 문헌은 찾을 수 없으며, 개인적 경험에 의존한 것으로 보인다. 정맥에서의 울혈성 출혈은 이러한 풍선압박으로 지혈이 될 수 있겠지만, 이는 압박 없이도 자연 지혈될 수도 있는 출혈일 수도 있다. 대표적인 기계적 지혈법은 상부 및 하부 위장관 출혈에 많이 사용되어 온 내시경 클립이 post-EST 출혈에도 사용될 수 있다[25,26]. 그러나 EST 후 발생한 출혈의 지혈을 위해 클립을 사용하는 경우 응고도자보다 더 출혈 부위에 적절한 접근이 어려우며, 클립이 측시경의 elevator를 지나면서 접히는 문제도 종종 생긴다. 그리고 잘못 결찰되거나 장내에 남겨진 클립이 지혈술을 방해하는 등의 문제도 생길 수 있으므로 주의가 필요하다. 식도정맥류 또는 위장관 출혈 지혈의 목적으로 사용되는 내시경 밴드결찰술도 성공적인 지혈 치료로 이용한 보고는 있지만, 췌장염과 담관 폐쇄의 위험이 높으므로 주의가 필요하다[27]. 최근 몇몇 보고에서 피막형 금속관(covered metal stent)을 총담관에 임시로 삽입하여 출혈 부위를 압박함으로써 효과적인 지혈을 보고하였다. 하지만 피막형 금속관이 고비용이 든다는 점과 다시 스텐트를 제거해야 불편함이 있으므로 에피네프린 주입 등 다른 치료가 실패하거나 용이치 않을 경우 시도해 볼 수 있다[28,29].
4. 혈관조영술 또는 수술적 지혈
혈관조영술을 통한 지혈술과 수술은 내시경 치료로 성공하지 못한 출혈에 대하여 비슷한 효과를 보고하고 있다[30,31]. 최근 복강경 수술의 발전으로 과거에 비하여 수술시간과 합병증의 변화가 있지만, 십이지장 유두부는 후복막에 위치한 기관으로 수술적 접근이 비교적 어려운 위치이다. 혈관조영술에 의한 색전술 또한 발전을 하여 83-100%의 지혈 성공률을 보이고 있다[1,31]. 따라서 수술에 비하여 덜 침습적인 혈관조영술을 신속하게 시행할 수 있다면 환자의 상황에 따라 수술보다 먼저 고려할 수 있다.
결 론
Post-EST 출혈은 드물지만 때론 심각한 문제가 발생할 수 있으며 적절한 지혈이 실패하는 경우 환자의 생명을 위협할 수 있다. 출혈을 완전히 예측할 수 없지만 위험인자에 대해 잘 알고 있어야 post-EST 출혈을 최소화할 수 있다. 출혈에 대해 내시경 지혈술을 시행할 경우 시술 자체에 의한 장천공, 췌장염 등의 합병증도 발생할 수 있으므로 시술자는 다양한 내시경 지혈술에 대해 잘 알고 상황에 따라 적절하게 시행할 수 있어야 한다. 지혈술로 인한 천공(지연형 천공을 포함한) 및 췌장염을 예방하기 위하여 가능한 담관 및 췌관에 스텐트가 삽입하는 것이 바람직하다. 그리고 위에 열거한 다양한 내시경 지혈법을 해부학적 위치와 환자의 상태를 고려하여 순차적으로 시행할 수 있다. 또한 최근 피막형 금속관 삽입에 의한 지혈술이 높은 성적으로 보고되고 있으므로 상황에 따른 고려가 필요하다. 그리고 내시경 지혈이 어렵거나 실패한 경우 과다 출혈에 의한 저혈량 쇼크를 막기 위해 적극적인 수액공급과 수혈은 물론 혈관조영술이나 수술 치료가 신속하게 이루어 질 수 있도록 다학제 간 긴밀한 협조가 필요하다.