약물 유발 급성 췌장염
Drug Induced Acute Pancreatitis
Article information
Abstract
약물 유발성 급성 췌장염은 상대적으로 드문 질환으로 알려져 있다. 특히 다른 원인의 췌장염과 구분되는 특징적인 소견이 없고, 실제 약제와 췌장염의 상관 관계를 증명하기는 어렵기 때문에 정확한 진단이 어렵고, 상세한 병력 조사와 더불어 항상 약제 유발 가능성을 의심하는 것이 정확한 진단의 첫 걸음이다. 약물 유발성 급성 췌장염은 기존 문헌 보고에서의 약제 투약 후 췌장염 발생까지의 잠복기와 재투약으로 인한 췌장염 재발을 기준으로 class I-IV로 분류된다. 일반적으로 class I과 class II 약물의 경우 췌장염 발생 가능성이 높기 때문에, 임상에서는 이들 약제를 중심으로 진단 및 치료가 이루어진다. 결론적으로, 임상의는 약물 유발성 급성 췌장염의 가능성을 주지하여야 하고, 특히 원인이 불명확한 급성 췌장염 환자의 진단과 치료에 있어 다른 췌장염 원인을 배제하면서 투약 병력을 확인하고 약물 유발성 췌장염을 감별 진단하는 것이 필요하다.
Trans Abstract
Drug induced acute pancreatitis (AP) is considered a relative rare disease. It has no distinguishing clinical features and physician may ignore the possibility of that due to lack of clinical recognition. Although estimates of the relative frequency with which drugs causes AP vary widely, there is a difficulty in proving the causal relationship between drug and pancreatitis. Therefore, a careful history taking and high index of suspicion is required for making a correct diagnosis. Drug induced AP is classified (class I-IV) based on previous literatures demonstrating the latent period and rechallenge reaction. Generally, class I and II drugs have the greatest potential for causing AP. In conclusion, physicians should be more aware of the possibility of drug induced AP in patients with unexplained AP and treat appropriately by discontinuation of the offending drugs. Besides, well designed epidemiological studies are needed to better define the frequency and specific risk of pancreatitis associated with any individual drug in Korea.
서 론
급성 췌장염은 췌장의 가역적인 염증성 질환으로 임상에서 흔하게 접할 수 있는 소화기 질환이다. 급성 췌장염은 대부분 담석과 알코올이 주요 원인이지만, 이 외에 대사성 질환, 췌장기형, 복부손상, 감염, 자가면역질환, 약물 등이 또 다른 원인으로 작용한다. 최근 고령 인구 및 만성 질환의 증가로 약제의 장기 복용이 늘고 있고, 이와 연관된 약물 유발 급성 췌장염이 보고되고 있다. 그러나 이러한 연구의 대부분은 증례 보고 또는 소규모 후향적 분석이기 때문에 정확한 기전 및 유병률은 추정하기 어렵고, 전체 췌장염의 약 0.1-1% 정도가 약물과 연관되는 것으로 추정된다[1-4]. 서구와 비교해 국내에서는 상대적으로 드문 질환으로 여겨져 왔으나, 최근에는 국내에서도 다양한 약물 유발 급성 췌장염이 보고되고 발생 빈도가 꾸준하게 증가하고 있는 추세이다. 따라서 원인이 불명확한 급성 췌장염은 반드시 투약 병력을 확인하고 약물 유발 췌장염을 감별 진단하는 것이 필요하다. 약물 유발 급성 췌장염의 정확한 진단을 위해서는 먼저 알코올, 담석, 자가면역성 췌장염, 외상, 고칼슘혈증, 고중성지방혈증 그리고 췌장 종괴 등의 다른 원인을 먼저 배제하여야 하고, 유발 약제 투여와 급성 췌장염의 시간적 선후 관계를 증명하고, 재투약을 통한 췌장염의 재발이 증명되는 경우 확진할 수 있다. 본 고찰에서는 국내의 증례 보고를 기반으로 다양한 약제와 연관된 약물 유발 급성 췌장염에 대해 기술하고자 한다.
본 론
1. 약물 유발 급성 췌장염 분류
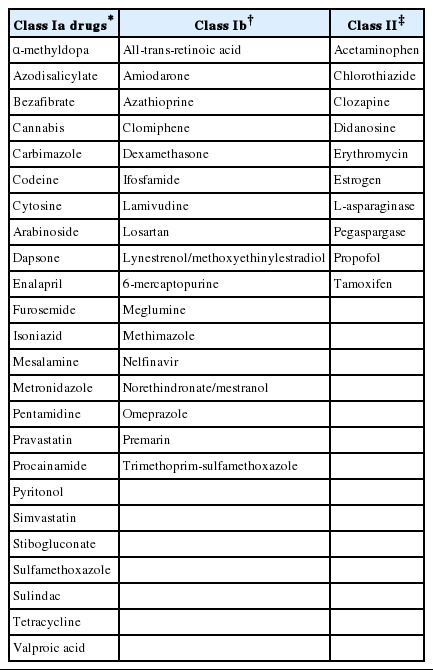
현재까지 약 120종 이상의 약물과 연관된 급성 췌장염이 보고되고 있으나, 대부분의 보고들은 단발성의 증례, 실제 약제 외의 다른 원인을 배제하지 않은 경우 또는 재투약을 통한 재발이 확인되지 않은 경우가 많아 실제 보고된 모든 약제가 췌장염과 연관되어 있다고 단정하기 어렵다. 이러한 제한점을 극복하기 위해 췌장염 연관 약제에 대한 증거 기반의 위험도 분류가 시도되었고, 2007년 Badalov 등[5]은 120개 약제를 문헌별 증거 기준을 수립하여 4가지 약제군으로 나누고, 약물 유발 췌장염의 원인을 분류하였다. Class I은 약물 재투약 후 급성 췌장염의 재발이 확인된 경우로, 이러한 약물 중 알코올, 고중성지방혈증, 담석 등의 다른 췌장염 원인이 완전히 배제되었다면 class Ia, 그렇지 않으면 class Ib로 세분화된다. Class II는 적어도 4편 이상의 증례 보고에서 투약과 급성 췌장염 발생 시 기간의 잠복기(latency)가 75% 이상 동일하게 보고된 약제이다. Class III은 2편 이상의 증례가 보고되었지만, 잠복기의 일관성이 없는 경우이고, class IV는 한 편의 증례 보고가 있었던 기타 약제이다.
사실 최근에는 초음파 내시경(endoscopic ultrasonography), 자기 공명 담췌관조술(magnetic resonance cholangiopancreatography) 등의 영상 의학 검사가 발전하고, 이전에는 개념이 명확하지 않았던 자가면역성 췌장염 등의 정의가 구체화되었기 때문에, 2000년대 초반 이전의 약물 유발 급성 췌장염 증례 보고들이 과연 정확한 진단이었는지 의문점이 있다. 그러므로 약물 유발 급성 췌장염의 진단에는 투약과 췌장염의 시간적 선후 관계 및 재현성의 측면이 가장 중요하기 때문에, 실제 임상에서는 class I과 class II 약물을 중심으로 진단 및 치료가 시 행된다(Table 1).
2. 임상적 특징
약물 유발 급성 췌장염의 발생 기전은 불명확하지만 과민성 반응(hypersensitivity reaction), 약 자체 및 대사 물질의 세포 독성, 오디 괄약근의 수축 유발 등의 기전으로 설명된다. 가장 흔한 기전은 과민성 반응(hypersensitivity reaction)으로 투약 4-8주 사이에 발생하고 용량과 연관성이 없다. 이 경우 약제 재투여시 수시간에서 수일 안에 급성 췌장염이 재발한다. 두 번째 기전은 독성 대사물질의 축적에 의한 급성 췌장염으로 투약 수개월 이후에 발생하는 경우에 해당한다. 약물 유발 급성 췌장염은 특징적인 임상 및 검사 소견이 없이, 다른 췌장염 과 동일하게 특징적인 복통, amylase/lipase의 상승과 영상 검사상 췌장의 부종 및 괴사 등의 췌장염 소견 등이 관찰된다. 일부 환자에서 발진, 호산구 증다증, 림프절 비대 등의 약제 과민성 반응 소견을 보일 수도 있지만, 독성 대사물질의 축적으로 수개월 후에 발생하는 경우를 비롯하여 대다수의 경우는 특징적인 임상 소견이 없다. 또한 대부분의 약물 유발 급성 췌장염의 예후는 약제를 중단할 경우 쉽게 호전되어 다른 원인에 의한 췌장염에 비해 양호하다[3,6].
3. 대표 유발 약제
1) Azathioprine, 6-mercaptopurine (6-MP): class Ib
Thiopurine계 항대사성 물질인 azathioprine과 그의 대사 물질인 6-MP는 급성 췌장염을 유발할 수 있다. 이러한 약제는 세포 독성 작용과 면역 억제 작용이 있기 때문에 장기 이식 또는 여러 자가면역질환에서 광범위하게 사용되고 있다. 일반적으로 췌장염은 azathioprine 투약 후 2개월 내에 발생하고, 투약을 중단하면 빠른 증상의 호전을 보인다. 국내에서도 궤양성 대장염, 크론병 등의 염증성 장질환과 류마티스 관절염, 베체트병에서 약물 유발 급성 췌장염이 보고되었다[7-9]. 특징적인 것은 용량과 관계없는 과민성 반응으로 인해 발생하게 되며, 국내 보고에서는 투약 3-4주 후 발생하고, 약제 중단 후 쉽게 호전되었다.
2) Mesalazine, sulfasalazine: class Ia
Mesalazine, sulfasalazine은 궤양성 대장염, 크론병 등의 염증성 장 질환에서 사용하는 약제로 경구 또는 좌약 제제로 사용된다. 궤양성 대장염 환자는 일반인보다 약 2배 이상 급성 췌장염의 발생 빈도가 증가하고, 장기간 약제를 사용하는 경우가 많기 때문에 환자가 급성 췌장염이 발생한다면 알코올, 담석 등의 일반적인 원인 외에도 항상 치료 약물에 의한 급성 췌장염을 의심할 수 있어야 한다[10]. 국내에서도 mesalazine, sulfasalzine 제제로 인한 약물 유발 급성 췌장염이 여러 차례 보고되었고, 특히 약물 재투여시 급성 췌장염이 재발하는 것 이 증명되었다[8,11,12]. 대부분의 보고에서 24-48시간에 급성 췌장염이 발생하고 약제 중단 후 호전되었고, 좌약의 경우도 경구약과 마찬가지로 급성 췌장염이 발생하였다.
3) Isoniazid: class Ia
일차 항결핵약제로 사용되고 있는 isoniazid는 드물게 급성 췌장염이 발생할 수 있다. Isoniazid 초기 투여 후 약물 유발 급성 췌장염은 0.5-21일까지 다양하게 발생된다. 국내에서도 두 편의 isoniazid 유발 급성 췌장염 증례 보고가 있었고, 한 예는 투약 시작 후 13일째 발생한 경증 급성 췌장염이었고, 다른 증례는 투약 5주 이후 발생한 가성 낭종 출혈을 동반한 중증 급성 췌장염이었다[13,14].
4) Methimazole: class Ib
그레이브씨병에서 사용되는 약제인 methimazole은 잘 알려진 위험한 부작용인 무과립구증(agranulocytosis) 외에도 약물 유발 급성 췌장염이 발생할 수 있다. 국내 보고에서는 51세 그레이브씨병 여자 환자에서 2주의 methimazole 투약 치료 후 무과립구증 없이 급성 췌장염이 발생하였고 재투여로 재발이 확인되었다[15].
5) Trimethoprim-sulfamethoxazole: class Ib
Trimethoprim-sulfamethoxazole은 sulfa 항생제로 요로 감염 및 human immunodeficiency virus 환자 등에서 많이 사용되고 있는 약제이다. 국내에서는 32세 남성 요도염 환자에서 3일간 투약 후 급성 췌장염의 발생이 보고되었고, 이 환자는 전립선염 2주 투약 치료 후 급성 췌장염의 기왕력이 있어서 약물 유발 급성 췌장염의 재발을 확인할 수 있었다[16].
6) Sulindac: class Ia
Sulindac은 흔하게 사용되는 비스테로이드성 항염증제 (nonsteroidal anti-inflammatory drug)로 prostaglandin 억제 효과가 적어 신독성은 적고 간독성이 높은 것으로 알려져 있다. 37세 여성 전신성 경화증(systemic sclerosis) 환자에서 투약 2주 후에 담즙 울혈성 간염과 급성 췌장염이 같이 발생한 국내 증례 보고가 있었다[17].
7) L-asparaginase: class II
L-asparaginase는 성인 급성 림프모구 백혈병 환자에 사용하는 항암제로 과민 반응, 고혈당, 간부전 등의 여러 가지 부작용이 보고되고 있다. 급성 췌장염은 치료 시작 2일 뒤부터 치료 중단 10주 뒤까지 나타날 수 있는 합병증으로, 국내에서는 20세 여자 pre-B 급성 림프모구 백혈병 환자에서 항암 치료 11일째 괴사를 동반한 중증 급성 췌장염이 발생하다[18].
8) Ciprofloxacin
Ciprofloxacin은 흔하게 사용되는 quinolone 계열 항생제로, Badalov의 분류에는 들어가지 않지만, 국내 단일 기관 연구에서 급성 췌장염과 약제의 상관관계가 확인되었다. 급성 감염성 장염 227명 중 3.1%에서 급성 췌장염이 진단되었고, 발생 시 ciprofloxacin 투약 평균 5.5일, 회복 기간은 약 11.3일이었다[19]. 상기 연구에서 복통, 혈청 amylase/lipase 상승, 복부 전산화 단층촬영을 통해 췌장염이 확인되었기 때문에 장염 이후 발생한 담즙 앙금(sludge) 및 미세담석(microlithiasis)과 연관된 급성 췌장염이 완전히 배제되지 못하고 치료 특성상 재투약이 이루어지지 못한 제한점이 있지만, 저자들은 특이 과민 반응(idiosyncratic hypersensitivity reaction)에 의한 약제 유발 급성 췌장염을 보고하였다.
9) DPP-4 억제제, GLP-1 유사체
Glucagon like peptide-1 (GLP-1)은 소장에서 분비되는 인크레틴 호르몬으로 췌장의 인슐린, 루카곤 분비를 조절한다. Sitagliptin, vildagliptin, saxagliptin 등의 dipeptidylpeptidase-4 (DPP-4) 억제제는 GLP-1을 분해하는 효소인 DPP-4 작용을 억제하여 인크레틴을 활성화하는 작용을 하는 경구 약제로 위장관 부작용과 체중 변화가 거의 없다. Exenatide와 liraglutide는 GLP-1 수용체작용제(receptor agonist)와 GLP-1 유사체(analog)로 혈당 강하 효과가 우수하고 체중 감소 효과가 있는 주사제이다. DPP-4 억제제와 GLP-1 유사체 모두는 저혈당 부작용이 적어 제2형 당뇨병의 혈당 강하제로 최근 사용이 증가하고 있지만, 기존 연구에서 췌장염과 췌장암 위험도의 증가가 보고되었다[20]. 사실 이러한 췌장염, 췌장암 위험도 증가는 아직 논란의 여지가 있지만[21,22], 적어도 약물 유발 급성 췌장염의 또 다른 원인 약제의 가능성이 있다. 당뇨병은 만성 질환으로 장기간 투약이 필수적이기 때문에 DPP-4 억제제와 GLP-1 유사체의 사용은 특히 유의하여야 한다[23,24].
4. 기타 약제
최근 임상에서 흔하게 진단하고 치료하는 고혈압, 고지혈증, 위십이지장 역류 등은 장기간 약물치료가 필요한 경우가 많기 때문에 투약에 주의를 요한다. 특히 약물 유발 급성 췌장염의 원인 약제 class Ia인 simvastatin/pravastatin, enalapril, valproic acid, furosemide 등과 class Ib인 omeprazole, losartan, lamivudine 등은 사용 전 췌장염 위험성을 항상 숙지하여야 하며, 장기간 투약에 주의하여야 한다. 그 외에도 다발성 골수종 치료제로 사용되는 프로테아좀 억제제인 bortezomib의 경우도 약물 유발 급성 췌장염이 보고되어 사용에 주의가 필요하다[25].
결 론
약물 유발 급성 췌장염은 매우 드물고 특징적인 소견이 없어 정확한 인과 관계의 증명과 임상 증상을 기반한 진단이 쉽지 않다. 그렇지만 임상의는 원인이 불명확한 급성 췌장염에 있어서는 약물 유발 급성 췌장염의 가능성을 항상 염두에 두고 진단과 치료적 접근을 하여야 하며, 항상 췌장염 유발 가능 약제 사용시 주의를 기울여야 한다.
Notes
Conflict of Interest
The author has no conflicts to disclose.