가성 낭종을 동반한 췌장의 동정맥 기형
Pancreatic Arteriovenous Malformation Combined with Pseudocysts
Article information
Abstract
췌장의 동정맥 기형은 주로 췌장의 두부에 생기는 매우 드문 질환으로 주 증상은 위장관 출혈이며, 치료는 일반적으로 침범된 기관 또는 부위의 완전 절제이다. 저자들은 급작스런 복통으로 내원하여 췌장미부에 동정맥 기형이 진단된 64세 남자 환자의 임상소견과 수술적 치료경과를 보고하고자 한다. 췌장 컴퓨터단층촬영과 자기공명담췌관 조영술 상에서 췌장 미부에 다발성의 혈관생성을 동반한 동정맥 기형에 합당한 소견이 관찰되었으며 인접한 근위부 췌장에 낭성병변 동반소견이 보였다. 같은 시기에 시행한 상장간막동맥 혈관조영술에서도 췌장미부에서 동맥영상 조기에 간문맥이 관찰되는 동정맥 기형 소견이 보였다. 치료는 복강경하 원위부 췌장 절제 및 비장 절제술을 시행하였으며, 조직검사에서 췌장 미부에 동정맥 기형에 합당한 소견과 근위부에 가성낭종의 소견이 보였다. 환자는 수술 후 1주만에 합병증 없이 퇴원하였다.
Trans Abstract
Pancreatic arteriovenous malformation (PAVM) is very rare anomaly. It occurs most commonly in the pancreatic head portion and gastrointestinal bleeding is the most common symptom. The management of PAVM is rather complex, with complete treatment usually accomplished by a total extirpation of the affected organ or at least its involved portion. We report the clinical presentation and management of 64 year-old male patient with PAVM, which was developed in pancreatic tail portion with sudden abdominal pain. Pancreatic computed tomography and magnetic resonance cholangio-pancreatography were consistent with a vascular formation on pancreatic tail portion and simultaneously revealed with pseudocysts beside it. A subsequent superior mesenteric artery angiographic findings depicted PAVM on pancreatic tail portion. The patient underwent laparoscopic distal pancreatectomy and splenectomy and had a favorable outcome.
서 론
췌장의 동정맥 기형(pancreatic arteriovenous malfomation)은 매우 드문 질환으로 1968년 Halpern 등[1]에 의해 처음 보고되었다. 국내에서는 2000년 Jang 등[2]에 의해 처음 보고된 이후로 몇 건의 산발적인 보고가 있었으며[3–6], 다양한 임상증상의 동반과 그에 따른 각기 다른 형태의 치료가 보고되었다. 병변은 주로 췌장 두부에서 호발하며 가장 흔한 증상으로는 소화관출혈(47.2%)과 이에 수반되는 복통(46.1%)이며, 합병증으로는 출혈(50.6%), 췌장염(16.9%), 문맥고혈압(6.7%), 가성 낭종(3.4%) 등이 나타날 수 있다[7]. 치료는 여러 의견이 있을 수 있으나 대부분의 경우에 있어 문맥압항진과 출혈위험이 있어 수술적 치료가 고려된다[7,8]. 복부통증을 주소로 한 64세 남자에게서 췌장 미부에 가성 낭종을 동반한 췌장 동정맥 기형이 발견되어 복강경 수술로 치료한 증례를 문헌고찰과 함께 보고하고자 한다.
증 례
64세 남자가 2주 전부터 시작된 복부 불편감과 3일 전부터 시작된 복통으로 외부 병원에서 복부 컴퓨터단층촬영을 시행받았으며 췌장의 종괴가 의심되어 본원 소화기내과로 의뢰되었다. 과거력상 1990년 충수돌기염으로 충수돌기 절제술을 시행한 이력 외에 기저질환 상의 특이사항은 없었고 음주는 주 1회 소주 1병, 흡연은 40 pack year의 과거력이 있었다. 전원 전 외부 병원에서 시행한 위 내시경, 대장 내시경 검사상 특이소견은 없었다. 내원 당시 혈압 137/83 mmHg, 체온 36.5°C, 맥박수 81회/분, 호흡수 20회/분이었으며 결막 창백이나 공막의 황달은 없었다. 흉부 청진에서 특이소견은 없었으며 규칙적인 심음이 관찰되었고 복부 진찰시 상복부 압통을 호소하였다. 말초혈액 검사에서 백혈구 12,880/mm3 (중성구 65.5%), 혈색소 15.1 g/dL, 혈소판 383,000/mm3, AST 12 U/L, ALT 13 U/L, ALP 100 U/L, GGT 46 U/L, total protein 7.1 g/dL, albumin 4.8 g/dL, total bilirubin 0.6 mg/dL, direct bilirubin 0.1 mg/dL였고, 전해질은 sodium 136 mmol/L, potassium 4.7 mmol/L, chloride 102 mmol/L였으며, 혈청 amylase 65 U/L, lipase 67 U/L, 종양표지자는 CA19–9 10.30 U/mL, CEA 2.64 ng/mL로 정상 범위 내에 있었다. 본원에서 시행한 췌장 컴퓨터단층촬영 및 자기공명췌담관 촬영에서 췌장미부에 경계가 불분명한 비균일적 조영증강이 보이는 부분이 관찰되었으며 이는 불규칙하게 확장된 소혈관들과 연결을 보이고 있었다(Fig. 1). 주위에는 2개의 작은 낭성 병변들도 관찰되었으나 췌장염의 소견은 없었다. 상부장간막혈관조영술상 췌장의 동일 부위의 동맥영상에서 췌동맥의 과혈관성이 보였으며, 조기 정맥영상에서 췌장 체부와 미부 경계 혈관 부위에서 문정맥배액이 관찰되었다(Fig. 2). 이상과 같은 소견을 종합하여 췌장미부(체부와의 경계 부위)의 동정맥 기형을 진단하고 복강경을 이용해서 췌장 체부를 포함한 원위부 췌장 절제술과 함께 비장 절제술을 시행하였다. 수술 후 조직학적 소견에서 동일 부위에 췌장 동정맥 기형에 합당한 소견이 관찰되었으며(Fig. 3) 주위의 낭성병변은 반투명의 액체 내용물이 있었으며 lining epithelium은 관찰되지 않아 가성 낭종으로 진단하였다. 환자는 수술 후 일주일 만에 합병증 없이 퇴원하였다.
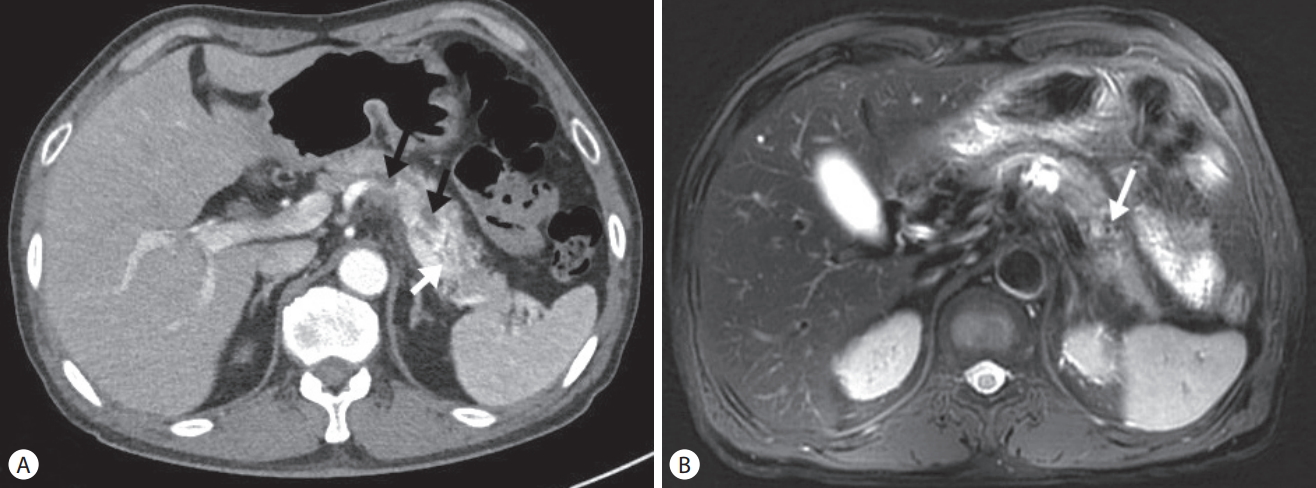
Contrast-enhanced pancreatic computed tomography (CT) scan and magnetic resonanace image (MRI). (A) Late arterial phase CT scans consistent with a vascular formation on pancreatic tail portion (white arrow) and simultaneously revealed with small pseudocysts besides it (black arrows). (B) In arterial phase MRI scan, heterogenous enhancement with unclear border and tortous dilated vessels with signal void in the T2 weighted image were observed (white arrow).

Superior mesenteric artery angiography (early arterial phase). Angiography showed increased vascularity at the pancreatic tail (black arrow) and early portal venous drainage through the pancreatic body and tail vessels (white arrow).

Histopathologic findings. (A) Postoperative resected gross specimen (pancreas and spleen) revealed with abundant vascularity. (B) A section of the specimen showed abundant and dilated arteries and veins (arteriovenous malformation). (C) Histopathologic examination of resected specimen showed varing mixture of dilated arteries and veins (H&E stain, ×130). (D) tortous and dilated arteries and veins are seen on the smooth muscle actin staining (SMA stain, ×300).
고 찰
동정맥 기형은 소화기관 내에서 드문 질환으로 간 또는 간 주위 부분에서 발생되는 경우가 가장 많으며 맹장을 포함한 우측 대장이 그 다음이다. 췌장에서의 동정맥 기형 발생은 전체 소화기관의 발생빈도에서 0.9%를 차지할 정도로 드문 질환이다[9].
따라서 국내에서의 췌장의 동정맥 기형도 매우 드물게 보고되고 있으며[2-6], 다양한 합병증이 병발하는 것으로 되어있다. 대부분 선천적으로 발생되고 그 원인은 확실치는 않으나 태아 맥관망에 의해 발생하는 것으로 추정하고 있으며, 후천적으로는 염증, 종양, 외상 등에 의해 이차적으로 발생된다고 알려져 있다[9]. 본 예에서는 종양, 외상, 췌장염 등의 뚜렷한 과거력이 없는 것으로 미루어 선천적인 것으로 생각되며 주변부의 가성 낭종은 동정맥 기형의 합병증으로 발생한 것으로 추정된다. 국내에 보고된 췌장 동정맥 기형 중 가성 낭종이 병합된 경우는 본 증례를 제외하고는 한 예에 불과하였다[6]. 호발 부위는 주로 두부에 나타나나 체부 및 미부에서도 발생할 수도 있다[3]. 무증상이 가장 흔하나 증상이 있는 경우에는 출혈이 가장 많고 그 외에 복통, 문맥압항진, 복강내 출혈, 췌장염 그리고 황달 등의 드문 증상도 나타난다[3,10]. 동정맥 기형에서 췌관으로의 출혈, 동반된 십이지장점막 동정맥 기형의 파열에 의한 출혈, 문맥고혈압으로 발생한 정맥류의 출혈, 동정맥 기형에 인접한 십이지장의 궤양에 의한 출혈 등이 출혈의 원인으로 알려져 있다[10]. 이 중 가장 흔한 원인은 문맥고혈압에 의한 정맥류출혈인 것으로 보고된다[11]. 출혈이 있다면 출혈의 원인을 찾기 위한 상부위장관 내시경 검사가 반드시 필요하다. 복통은 장간막혈관의 혈류순환으로부터 혈액이 동정맥 기형을 통해 바깥쪽으로 빠져나가는 스틸 증후군에 의해 유발되는 것으로 생각된다[8,12]. Chou 등은[7] 89명의 췌장 동정맥 기형을 분석한 결과 두부에 위치한 병변에서 체부와 미부에 위치한 병변에 비해 약 2배가 넘는 비율로 출혈을 동반하는 것으로 보고했다. 반면 췌장염의 경우 체부와 미부에 위치한 병변에서 두부에 비해 3배에 가까운 비율로 동반되는 것으로 보고하였다.
췌장 동정맥 기형시에 나타날 수 있는 췌장염에 대한 기전은 확실히 밝혀진 바는 없으나 동정맥 기형으로부터의 출혈이 췌관으로 퍼지거나 빠져나간 혈류가 주위 췌장 조직에 허혈성 손상을 야기할 수 있으며 동정맥 기형 자체의 췌관 압박 가능성 등을 추정하고 있다[13]. 췌관 압박에 의한 췌장염과 가성 낭종의 발생은 장액성 낭종에서도 발생한다는 보고도 있다[14]. 본 증례에서 나타난 췌장 동정맥 기형 주변부의 가성 낭종은 이러한 췌장염의 기전에 기인하여 발생한 것으로 추정된다.
췌장 동정맥 기형 진단은 컴퓨터단층촬영, 자기공명영상, 혈관조영술, 초음파 검사 등의 영상학적 방법으로 진단을 하게 된다. 감별진단은 낭포선암, 혈관육종 및 췌장세포종양 등이 있다. 확진을 위한 방법으로 혈관조영술을 이용하게 되고 그 특징적인 소견은 구불구불한 영양동맥, 포도송이 모양의 췌장내 혈관 구조물, 간문맥의 조기조영 그리고 췌장조영의 빠른 소실 등이다[10]. 혈관조영술은 합병증으로 온 출혈의 조절을 위한 색전술 시행에도 이용될 수 있다. 이 외에 비침습적 방법으로 컬러도플러 초음파를 이용한 진단방법도 소개되어 주목받고 있다. 그러나 위와 식도의 공기음영이 있는 경우 관찰이 어렵고, 술자의 숙련도가 검사 결과에 영향을 줄 수 있다는 단점이 있다[15]. 최근 영상기술의 발전으로 침습적인 혈관조영술을 대신해서 병변 내에 박동성 혈류를 볼 수 있는 도플러초음파와 다발성 과혈관 부위를 보여주는 컴퓨터단층촬영 혈관조영술, 다발성의 신호공백으로 나타나는 둥근 병변을 보여주는 자기공명영상 등이 비침습적인 진단의 도구로 더 선호되는 추세이다[7]. 허나 아직까지 병변의 크기를 정확히 파악하고 치료방향 및 수술방법을 결정하는 도구로서 혈관조영술이 더 특징적인 것으로 알려져 있다[11-13]. 즉, 진단 이후 근치적 치료의 세부적인 방법을 결정하는데 있어서 중요한 역할을 한다. 본 증례에서는 동정맥 기형의 크기를 감안할 때 수술적 치료가 합당하다고 판단되었으며 이상혈관(aberrant vasculature) 구조를 확인하기 위하여 혈관조영술을 시행하였다.
치료는 크게 수술적 치료와 비수술적 치료가 있다. 수술이 어려운 환자의 경우에서 급성 출혈을 막기 위한 방법으로 경도관색전술을 이용하여 영양혈관이나 유출정맥을 막아 치료를 한 경우에 대한 보고도 있다[5,15]. 하지만 시술이 어려울 뿐 아니라 장이나 주변조직의 괴사 위험성이 크고 술기 후에도 재발 및 재출혈, 문맥고혈압으로 진행 등의 문제가 발생할 수 있다. 또한 문맥압항진이 진행된 경우에는 수술 후에도 문맥압의 호전은 어려운 것으로 되어있기 때문에 진단이 되면 빠른 수술적 치료가 고려되어야 한다[8,9]. 수술의 경우 췌장두부의 병변은 췌십이지장 절제술을, 그 이외의 경우에는 원위부 췌장절제술을 시행하게 된다[8].
저자들은 복통을 호소하는 환자에게서 컴퓨터단층촬영, 자기공명영상, 혈관조영술의 방법을 이용하여 췌장의 낭종을 동반한 췌장 미부의 동정맥 기형을 진단하였고 복강경 수술을 통해 치료를 하였다. 췌장의 동정맥 기형 중 두부에 생기지 않고 출혈을 동반하지 않는 형태로 본 증례처럼 복통의 증상과 낭종을 동반한 미부의 동정맥 기형은 매우 드물다. 이에 원인이 명확하지 않은 복통을 호소하는 환자에서 드물기는 하지만 췌장 동정맥 기형을 감별질환으로 고려해야 할 것으로 사료되어 본 증례를 보고한다.
Notes
Conflict of Interest
The authors have no financial conflicts of interest.