간절제술 후 간내담석 관련 합병증에서 피부간경유쓸개관조영술의 효과 및 경과
Effect and Course of Percutaneous Transhepatic Cholangioscopy in Intrahepatic Stone Related Complication after Liver Resection
Article information

Abstract
배경/목적
간내결석으로 간절제술 시행 후 재발한 경우, 주로 피부간경유쓸개관조영술(PTCS)로 치료하는데 이런 PTCS의 효과 및 경과에 대한 연구는 거의 없다. 이에 간절제술 후 간내결석 관련 합병증이 발생한 환자에서 PTCS의 효과 및 경과에 대해서 보고한다.
방법
1998년 1월부터 2014년 12월까지 삼성서울병원에서 간내결석으로 수술 후 PTCS를 시행한 19명의 환자를 대상으로 후향적 연구를 시행하였다. PTCS 시행 전 환자 특성, 시술 후 결석의 제거 여부 및 합병증, 경과 관찰 중에 재발 여부 등에 대해서 조사하였으며, 시술 후 간내결석의 재발과 관련된 요인에 대한 분석을 하였다.
결과
PTCS의 적응증은 담관염(12/19, 63.2%), 복통(3/19, 15.7%), 간농양(2/19, 10.5%), 담관 확장(2/19, 10.5%) 등의 급성 합병증이었으며 이러한 급성 합병증은 치료 후 모두 호전되었다. PTCS 시행 후 63.2% (12/19)에서 간내결석이 완전히 제거되었고, 평균 4.9년(범위, 1.8-7.8)의 추적관찰 기간 동안에 간내담석 관련 합병증이 52.6% (10/19)에서 발생하였다. 합병증은 담관염 5명(50%), 담관염 및 간농양 3명(30%), 간 농양 1명(10%), 복통을 동반한 결석 1명(10%)이었다. 재발과 관련된 요인으로 결석의 다발성, 완전 제거 여부, 담관 협착 등을 분석하였으나 합병증 재발과 통계적으로 유의한 관련성이 없었다.
결론
PTCS는 간내결석으로 간절제술을 받은 환자에서 재발된 간내결석의 급성 합병증에 효과적인 치료 방법이다. 그러나 PTCS로 결석 치료 후에도 간내결석의 재발 및 급성 합병증이 흔하게 발생하므로 추적관찰이 필요하다.
Trans Abstract
Background/Aims
Percutaneous transhepatic cholangioscopy (PTCS) is an effective treatment used for intrahepatic stone in patients who have undergone hepatectomy. There are few reports on natural course in these patients. Thus, we report the long-term results.
Methods
We conducted a retrospective study of 19 patients who underwent PTCS after hepatectomy at Samsung Medical Center between January 1998 and December 2014. We investigated patient characteristics and recurrence of biliary complications during follow up period. Then, we analyzed the factors related to recurrence.
Results
Indications for PTCS were cholangitis, symptomatic stone, liver abscess and biliary dilatation. Complete stone removal was achieved in 12 patients (63.2%). After receiving PTCS, the recurrence of intrahepatic stone related complication occurred in 52.6% (10/19) of patients during a median follow-up of 4.9 years (range, 1.8-7.8). Complications were cholangitis (5/10, 50%), cholangitis with liver abscess (3/10, 30%), liver abscess (1/10, 10%) and symptomatic stone (1/10, 10%). On univariate analysis, factors including multiple stone involvement, complete stone removal and bile duct stricture were not significantly associated with recurrent biliary complications.
Conclusions
PTCS is an effective treatment for complications of recurrent intrahepatic stones in patients who have undergone hepatectomy. However, long term follow-up is necessary because of the recurrence of biliary complications.
서 론
간결석증은 동아시아에서 흔한 질환으로 반복되는 담관염, 담도 협착, 간농양, 간경변, 간 위축, 담관암을 포함한 여러 합병증을 유발하는 것으로 알려져 있다[1-3]. 이러한 간결석증의 초치료로 간절제술과 피부간경유쓸개관조영술(percutaneous transhepatic cholangioscopy, PTCS)이 단독 또는 병행하여 시행되고 있다[4,5]. 일반적으로 근치적 목적으로 주로 간 위축, 국소 결석, 담도 협착을 동반한 환자에서는 간절제술이 우선적으로 시행된다[6]. 이러한 수술적 치료를 받은 환자에 대한 장기간 관찰 연구 결과에서 간내결석의 완전 제거율은 83.3%이고 재발률은 30.9%로 보고되었다[5].
간절제술 시행 후 간내결석이 재발하면 담관염 및 간농양 등과 같은 합병증이 발생하는데, 이전 수술 후 남아있는 잔존 간을 고려할 때 추가적인 수술이 어려워서 이러한 환자들은 주로 PTCS로 치료를 받게 된다[5]. 1차적 치료로 시행한 수술[5,7,8] 및 PTCS [5,9,10]에서 장기 추적 결과에 대한 보고는 있으나 간절제술 후 재발되어 PTCS를 시행받은 환자들에서의 장기간 추적관찰결과에 대한 보고는 거의 없다.
본 연구에서는 간내결석으로 간절제술을 시행받은 후에 재발하여 PTCS를 받은 환자들에서 장기간 추적관찰한 경과를 알아보고, 수술 후 PTCS 시행한 환자에서 간내결석의 재발과 관련된 인자를 확인하고자 한다.
방 법
1. 연구 형태 및 대상자
1998년 1월부터 2014년 12월까지 삼성서울병원에서 PTCS를 시행한 291명의 환자 중 PTCS 전에 간내결석으로 간절제술을 시행받은 19명의 환자를 찾아서 후향적으로 조사하였다. 본 연구의 진행은 헬싱키 선언에 따라 수행되었으며, 삼성서울병원기관윤리심의위원회의 승인을 받았다(IRB No. 2017-03-079).
2. 방법
대상 환자의 시술 전 특성과 PTCS 적응증, 재발한 간내결석의 위치 및 분포, 담도 협착 동반 여부, 결석의 완전 제거 여부를 확인하였다. PTCS 시행 후 간내담석 관련 합병증의 재발 여부를 확인하고 재발과 관계된 요인에 대하여 분석하였다. 이를 위하여 환자의 연령, 성별, 경피경간 담즙 배액(percutaneous transhepatic biliary drainage, PTBD) 유지 기간, 우르소데옥시콜산 사용 여부 등을 조사하였다.
합병증 을 동반한 간내결석은 담관염, 간농양, 통증을 동반하는 결석으로 복부 초음파(abdominal ultrasonography, US) 또는 컴퓨터단층촬영술(computed tomography, CT)을 통하여 확인하였다. 담관염은 38.3도 이상의 발열, 오한, 복통, 백혈구, C-반응성 단백질(C-reactive protein)과 같은 염증 수치의 증가, 간기능 이상 등을 토대로 임상적으로 진단하였다. 간농양은 US, CT상 농양에 합당한 영상 소견이 있고 복통, 발열 등의 감염에 합당한 임상 증상 및 증후가 있는 경우에 진단하였다. 결석과 관련된 복통은 다른 명확한 원인 없이 US 또는 CT상 간내결석을 보이면서 중등도 이상의 복통을 호소할 때 합병증으로 복통을 동반한 결석으로 정의하였다. 결석 위치는 첫 번째 우측 분지의 간내담관(right-sided first order intrahepatic duct, B1), 첫 번째 좌측 분지의 간내담관(left-sided first order intrahepatic duct, B2) 및 총담관으로 분류하였다.
PTCS는 다음과 같은 순서로 진행되었다. PTCS 전에 접근이 가능하면서 결석 제거가 쉬운 부위를 고려하여 6-8.5 Fr의 PTBD를 초음파와 투시 영상의 유도 하에 시행하고 삽입 후 약 1주 후에 확장기(dilator)를 사용하여 18 Fr까지 확장하였다. 추가로 약 1주일의 안정화(maturation)를 기다린 후, 간내결석의 제거를 위하여 PTCS가 시행되었다. PTCS 시행 시 PTBD를 넣은 담관 및 진입 가능한 담관의 결석은 모두 제거하였다.
3. 통계 분석
재발성 담석 관련 합병증과 관련된 요인을 확인하기 위하여, 연속변수의 경우, t -검정 또는 Mann-Whitney U test를 실시하였고, 범주형 변수의 경우, 카이제곱검정 또는 Fisher's exact test를 사용하여 분석하였다. 모든 분석에서 p -value가 0.05 미만인 경우 통계적으로 유의한 것으로 간주하였다. 모든 통계분석은 SPSS Statistics version 23 (SPSS Inc., Armonk, NY, USA)로 시행되었다.
결 과
1. 환자 특성
Table 1에 환자 특성에 대하여 정리하였다. 19명의 환자의 평균 연령은 60세(범위, 54-68)였고, 남자가 36.8%를 차지하였다. 좌외분엽절제술(left lateral segmentectomy), 좌측 반간절제술(left hemihepatectomy)은 13명(68.4%), 우측 반간절제술(right hemihepatectomy)은 6명(31.6%)에서 시행되었다. 수술 이후 간내결석과 관련된 합병증이 발생하기까지 평균 기간은 2.6년(범위, 1.6-6.0)이었다. PTCS의 적응증은 담관염(12/19, 63.2%), 복통(3/19, 15.7%), 간농양(2/19, 10.5%), 담관 확장(2/19, 10.5%)이었다. PTCS 시행 시 간내결석이 2개 이상의 분엽에 있는 환자는 13명(68.4%)이었고 담관 협착은 6명(31.6%)에서 관찰되었다(Table 1).

Baseline characteristics of study population
2. PTCS의 치료 효과 및 간내결석 관련 합병증 재발
PTCS를 시행한 19명의 환자에 대하여 Table 2에 정리하였고, 모두에게서 간내결석과 관련된 합병증은 PTBD 시행 후 3일 이내에 해결되었다. 19명 환자의 PTBD의 평균 유지 기간은 16일(범위, 14-22)이었다. 합병증 호전 후 PTCS를 시행하였고 2개 이상의 분엽의 간내결석에서도 해부학적으로 접근 가능하여 완전 제거할 수 있었던 6명을 포함하여 총 12명(63.2%)의 환자에서 완전 제거되었다. 완전 제거하지 못하였던 7명의 원인으로 원위부 말단 가지에 있던 경우(4명), 협착(2명), 심한 예각(1명)이었다.
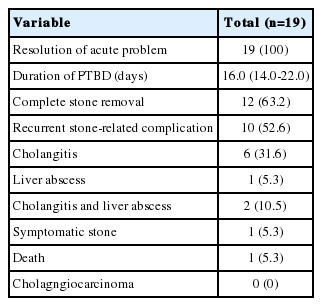
Clinical outcome of patient receiving PTCS for complication related hepatolithiasis
이후 평균 4.9년(범위, 1.8-7.8)의 추적관찰 기간 동안 10명(52.6%)에서 결석 관련 합병증이 재발하였다. PTCS 후 잔류 결석이 있던 7명 중 4명(57%)이 잔류 결석 관련 합병증이 발생하였으며 완전 제거되었던 12명 중 6명(50%)에서 간내결석이 재발하였고 모두 합병증이 발생하였다. PTCS 후 합병증이 발생하기까지 기간은 평균 55.0개월(범위, 10.9-1-14.0)이었다. 재발한 10명의 환자 중 5명(50%)이 담관염, 3명(30%)은 담관염 및 간농양, 1명(10%)은 간 농양, 1명(10%)은 복통을 동반한 결석이 발생하였다. 모두 항생제가 투여되었으며 이 중 간내결석 제거를 위하여 4명에서 PTCS가 시행되었고, 총담관결석과 간내결석이 동시에 존재하는 2명에서 내시경역행담췌관조영술(endoscopic retrograde cholangiopancreatogarphy)을 시행하였다. 이 중 1명은 PTCS 후 반복적인 담관염 및 간농양으로 항생제 치료를 받았으며 6년 후에 패혈성 쇼크로 사망하였다. Table 3에 PTCS를 받은 후 간내결석 관련 합병증이 발생한 환자 10명의 임상적 특성을 요약하였다.

Clinical characteristics of patients with recurrent biliary stone-related complication after PTCS
3. PTCS 후에 간내결석과 관련된 합병증 발생과 관련된 요인
재발성 담석 관련 합병증과 관련된 요인을 찾기 위해서 시행한 단변량 분석(univariate analysis)에서 나이, 성별, 결석의 다발성, 결석의 완전 제거 여부, 우르소데옥시콜산 사용 여부, 담관 협착 등과 합병증 발생과는 유의한 관련성이 없었다(Table 4).

Univariate analysis of risk factor associated with recurrent biliary stone-related complication after PTCS in patients having had hepatic resection
고 찰
본 연구에서 간내결석으로 간절제술 을 시행받은 후에 재발하여 다시 PTCS를 받은 환자 19명 중 12명에서 간내결석이 완전히 제거된 것을 확인하였고, PTCS 후의 추적관찰 기간 동안 10명의 환자에서 결석 관련 합병증이 재발한 것을 확인하였으나 이러한 재발과 관련된 요인은 발견되지 않았다.
간내결석에 대한 첫 치료로 PTCS를 시행한 이전 연구에 의하면 전체 환자 중 63.9%에서 결석의 완전제거가 보고되었다[5]. 간내결석으로 수술 후 재발한 환자에서 PTCS 시행한 본 연구에서도 비슷하게 63.2% (12/19)에서 완전하게 결석이 제거되었다. 간내결석으로 간절제술 후 재발한 환자에서도 PTCS가 수술받지 않은 환자에서만큼은 효과적인 치료임을 시사한다.
일반적으로 간내결석은 치료 후에도 재발하는 비율이 높은데, 이전 간내결석의 첫 치료로 PTCS를 시행한 연구들에서는 관찰기간에 따라 다양한 재발률(32.6-63%)을 보이고 있다[10-12]. 본 연구에서 확인한 간절제술 후 PTCS를 시행한 환자의 간내결석 관련 합병증의 재발률도 52.6%로 이전 절제술을 받지 않고 PTCS를 받은 환자와 비교할 때 상대적으로 재발률이 높은 군과 비슷한 재발률이 관찰되었다. 재발까지 평균 55.0개월(범위, 10.9-114.0)이었고 다양한 시기에 발생하는 것을 고려할 때, 장기간의 추적관찰이 중요하겠다.
간내결석으로 수술 또는 PTCS를 시행한 환자들의 재발에 비수술적인 치료, 담즙성 간경변, 잔류 결석, 담관 협착이 관련되어 있다고 보고하였지만[5], 간내결석으로 수술 후 재발되어 PTCS 시행한 환자를 대상으로 한 본 연구에서는 재발과 관련된 요인을 확인하지는 못하였다.
본 연구에서는 몇 가지 제한점이 있다. 연구에 포함된 환자의 수가 적었고 후향적으로 연구가 진행되었으며 환자마다 추적관찰 기간의 차이가 있다는 점이다. 이러한 한계로 간내결석 관련 합병증의 재발과 관련된 요인을 확인하기는 어려웠는데, 간내결석의 2개 이상의 분엽 침범(8/10, 80% vs. 5/9, 55%) 및 담도 협착(4/10, 40% vs. 2/9, 22%)은 재발과 높은 경향성을 보이고 있어 향후 더 많은 수의 환자를 포함하거나 전향적인 연구가 필요할 것으로 생각이 된다.
결론적으로, PTCS는 간내결석으로 간절제술을 받은 환자에서 재발된 간내결석의 급성 합병증에 효과적인 치료방법이다. 그러나 PTCS로 결석 치료 후에도 간내결석의 재발 및 급성 합병증이 흔하게 발생하므로 추적관찰이 필요하다.
Notes
Conflict of Interest
The authors have no conflicts to disclose.