췌장낭종의 영상의학적 평가와 감별 진단
Pancreatic Cystic Neoplasm: Radiologic Evaluation and Differential Diagnosis
Article information

Abstract
췌장낭종은 임상적으로 그 중요성이 점점 증가하고 있는 질환이다. 그 원인은 최근 영상 진단 기법의 발달과 잦은 검사로 인하여 발견이 매우 증가하고 있으며 일부 낭종은 악성 종양의 가능성이 있기 때문이다. 따라서 악성화 이전에 발견하여 적절한 추적관찰과 치료를 하는 것이 중요한데, 그 출발은 정확한 진단이다. 따라서 본고에서는 각 형태에 따른 감별진단을 다루고, 악성을 시사하는 소견에서 영상의 역할과 한계를 고찰하고자 한다.
Trans Abstract
Pancreatic cystic neoplasm is a clinically challenging entity. Its incidence estimated up to 45% of the general population. The biological behavior ranges from benign to malignant disease. The strategy for pancreatic cystic neoplasm could be to prevent progression to pancreatic cancer while minimizing the costs. The first step for the correct management is correct diagnosis. In this paper, the radiological differential diagnosis of them will be described.
서 론
췌장의 낭성종양은 두 가지 측면에서 임상적으로 아주 중요하다. 하나는 최근 영상 기법의 발달로 인하여 그 발견이 급속히 증가하면서, 일부에서는 일반 인구의 45%까지 보고하고 있다. 또 다른 측면에서는 간의 낭성종양과는 다르게, 생물학적 행동(biological behavior)이 양성에서 악성까지의 넓은 스펙트럼을 갖고 있다는 것이다. 따라서 동일한 낭성종양이라 할지라도 그 안에서 악성도의 정도에 따라 치료 방향이 달라질 수밖에 없다. 그 첫 번째 스텝은 정확한 진단이다. 우선 췌장의 여러 낭성종양을 감별 진단하고 그 안에서 악성도 유무를 판가름해야 한다.
췌장에서 감별 진단해야 하는 낭성종양으로는 가성낭종(pseudocyst), 장액성 낭종(serous cystic neoplasm, SCN), 점액성 낭종(mucinous cystic neoplasm, MCN), 췌관내유두상점액종양(intraductal papillary mucinous neoplasm, IPMN), 고형 종양의 낭성 변화(cystic change of solid tumor) 등이 있다. 본고에서는 이상의 병변에 대한 영상의학적 감별 진단의 실마리(clue)를 공유하고, 특히 화두가 되고 있는 IPMN의 악성도 예측에 대한 내용을 공유하고자 한다.
본 론
1. 췌관내유두상점액종양
IPMN은 1996년 세계보건기구에 의해 “an intraductal mucinproducing neoplasm with tall, columnar, mucin-containing epithelium, with or without papillary projection”으로 정의되었다. 형태학적으로는 주췌관형(main-duct type), 분지형(branch-duct type) 그리고 혼합형(mixed type)으로 분류되고 있고, 조직학적으로는 선종(adenoma), 경계성 종양(borderline malignancy), 상피내암(carcinoma in situ), 침윤성 종양(invasive carcinoma)으로 양성에서 악성까지의 스펙트럼을 보이는 낭성종양이다.
2017 Fukuoka 가이드라인은 주췌관형 IPMN을 “segmental or diffuse dilatation of main duct >5 mm, without other causes of obstruction”으로 정의하였다. 특이도를 유지하면서 민감도를 높이기 위하여 진단 기준을 이전의 1 cm에서 5 mm로 완화하였다[1]. 주췌관형 췌관내유두상점액종양에서 악성 종양의 비율은 44.9%까지 보고되고 있는데, 벽 결절(mural nodule; odds ratio [OR] 7.6)과 림프절(OR 3.8)이 악성 종양을 시사하는 영상 소견으로 보고되고 있다[2,3]. 영상학적 감별 진단을 요하는 질환은 만성 췌장염(chronic pancreatitis)과 췌장암(pancreatic ductal adenocarcinoma)이 있을 수 있다. 만성 췌장염에 의한 담관 확장은 대부분 다발성 협착(multifocal stricture), 췌관 결석(pancreaticolithiasis)이 동반되며 만성 췌장염의 기왕력이 존재하므로 감별 진단이 가능하다. 췌장암이 췌관 확장만으로 보일 때 감별 진단이 어려울 수 있으나, 하류췌관 확장(down-stream duct dilatation)이 있고 협착이 없는 경우 IPMN을 좀 더 시사한다고 할 수 있다.
분지형 IPMN은 낭종의 직경이 5 mm 이상이면서 주췌관과 교통이 있는 경우로 정의하고 있다(가성낭종을 제외) [1]. 분지형 IPMN의 영상 소견은 낭종의 모양이 포도양(grape-like), 다형성(pleomorphic), 또는 낭종외 낭종(cyst by cyst), 다방성 낭종(multilocular cyst)이면서 췌관과 교통이 있으면 진단할 수 있으며, 점액성 낭종, 장액성 낭종 등과의 감별 진단이 필요하다(Fig. 1). 분지형은 주췌관형보다 악성 종양의 비율이 현저히 낮아서 13.3%까지 보고되고 있으며, 벽 결절이 유일한 악성을 예측할 수 있는 소견으로 보고되고 있다(OR 9.2) (Fig. 2) [2,3]. 아시아와 유럽 가이드라인은 공통으로 수술의 절대적 적응증, 혹은 high risk stigmata로 폐쇄성 황달, 조영 증강되는 벽 결절(enhancing mural nodule) >5 mm, 주췌관 직경 >10 mm을 들고 있다[1,4]. Worrisome features 혹은 수술의 상대적 적응증으로는 약간씩 차이가 있는 많은 소견을 제시하고 있다. 두 가이드라인 공통으로는 조영 증강되는 벽 결절 <5 mm, 주췌관 직경 5-9 mm, 혈청 CA19-9 상승(37 U/mL), 낭종 성장속도(cyst growth rate) >5 mm/2년(1년), 낭종의 크기 >3 cm (4 cm)를 제시하고 있다. 그 외에, 낭종벽이 두꺼워지거나 조영 증강되는 경우, 림프절 종대(lymphadenopathy), 주췌관 직경의 갑작스러운 변화 및 원위부 췌장 위축, 새로 발생한 당뇨 그리고 IPMN에 의한 급성 췌장염 등이 있다[1,4].
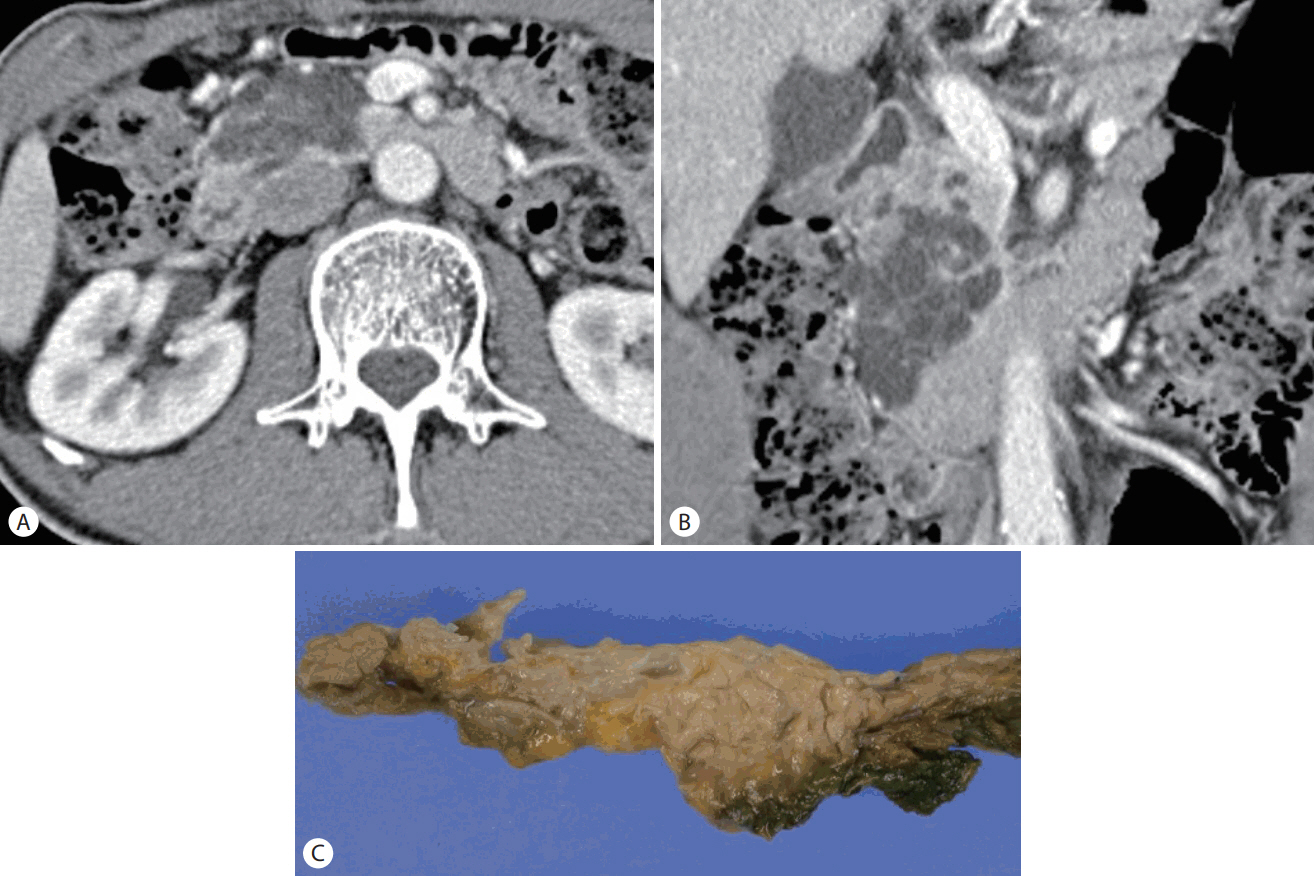
Intraductal papillary mucinous neoplasm (IPMN), adenoma. (A, B) Axial and coronal contrast-enhanced computed tomography scan shows a cluster of pleomorphic cysts separated by thin septa. (C) Gross specimen shows IPMN, branch-duct type, adenoma.
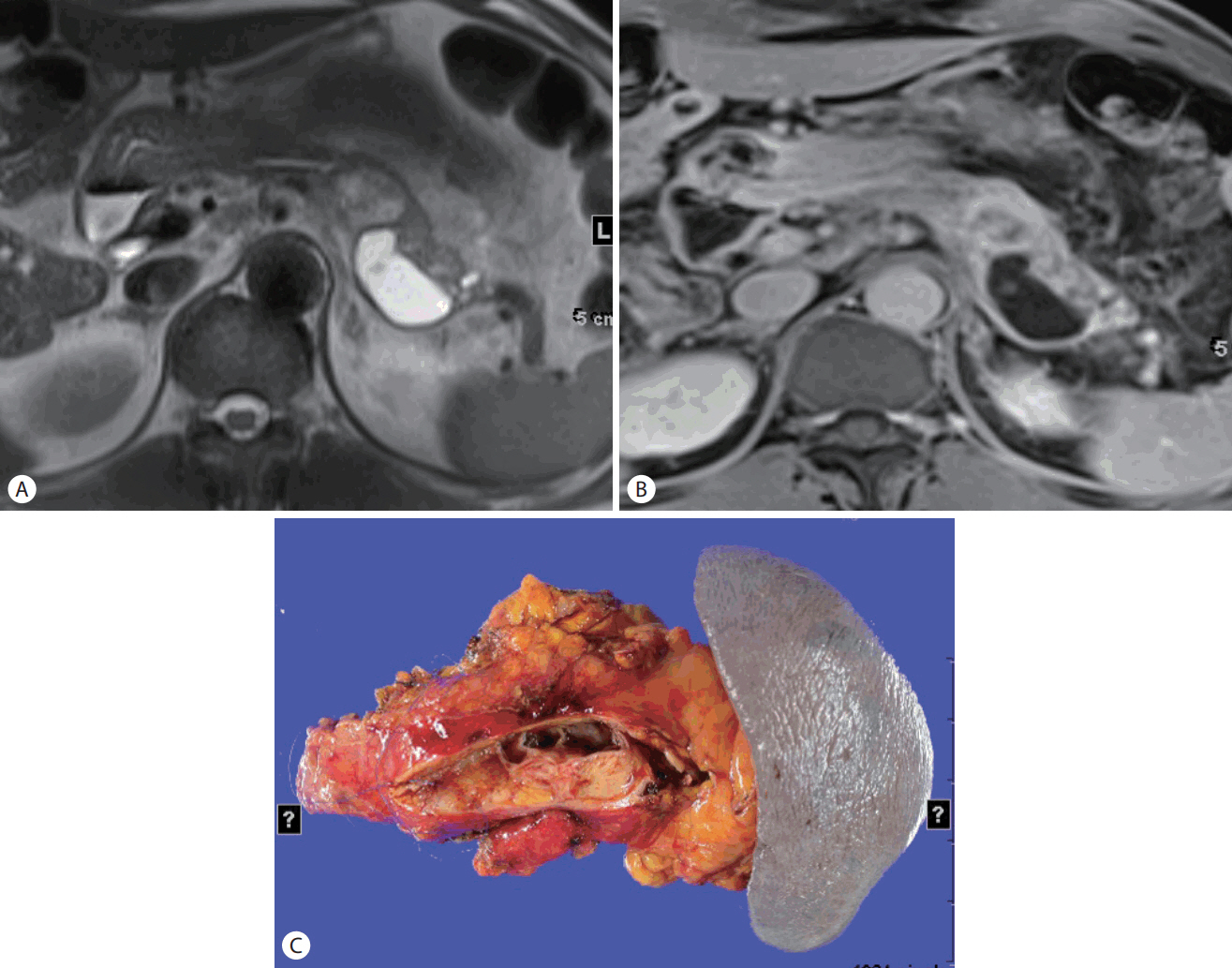
Intraductal papillary mucinous neoplasm (IPMN), invasive. (A) T2-weighted magnetic resonance image (MRI) shows cystic and solid mass at the body and tail of the pancreas. (B) Contrast-enhanced T1-weighted MRI shows enhancing solid mass combined with cyst. (C) Gross specimen shows IPMN, invasive.
2. 장액성 낭종
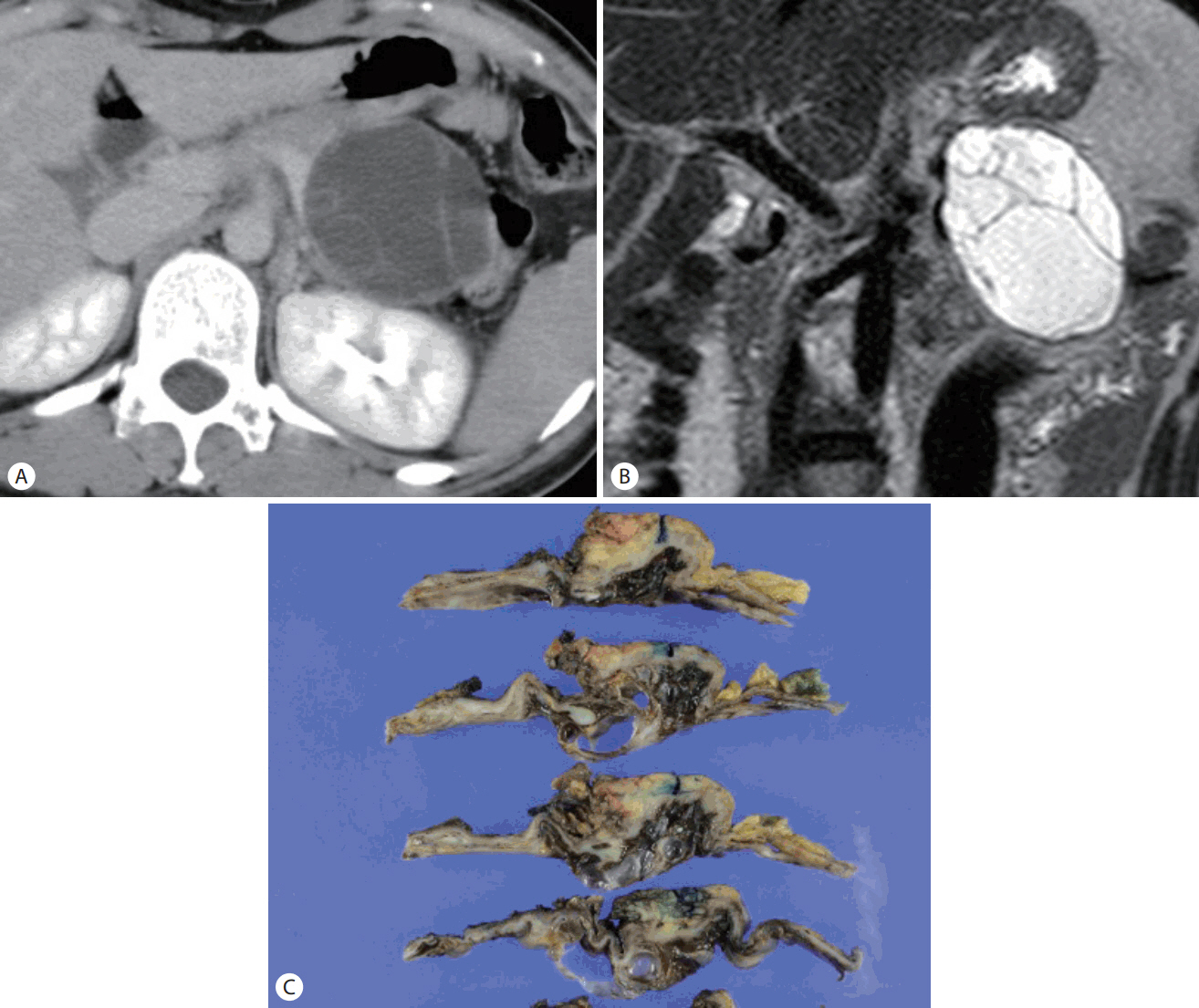
SCN은 양성 낭종이기 때문에 악성 가능성이 있는 IPMN, MCN과는 달리 수술이 필요치 않아서 정확한 진단이 중요한 낭종이다. 전형적인 영상 소견은 해면체(spongy) 또는 벌집모양(honeycomb-like), 소낭성(microcystic), 다방성(multilocular) 낭종이나 종종 대낭성(macrocystic)과 혼합된 형태로 보이며, 가끔 대낭성으로만 보일 경우도 있다. 중심부 석회화(central scar, central calcification)가 있는 경우 매우 특이적으로 진단할 수 있다(Fig. 3). SCN의 낭종은 매우 작은 낭종으로 구성되어 조영 증강 computed tomography (CT)나 magnetic resonance image (MRI)에서, 과혈관성의 고형 종괴처럼 보이는 경우가 종종 있다. 이 경우에는 신경내분비 종양(neuroendocrine tumor) 등과 감별이 필요한 경우가 있는데, T2-weighted MRI나, endoscopic ultrasound (EUS) 등에서 작은 낭종을 관찰하면 SCN을 진단할 수 있다. SCN이 대낭성낭종(macrocyst)으로 주로 구성되어 있는 경우에는 IPMN과의 감별이 어려운 경우가 종종 있다. 이 경우에 낭종의 모양이 다형성(pleomorphic)이거나 주췌관과의 교통이 있으면 SCN을 배제할 수 있고, 중심부 석회화가 있는 경우는 SCN을 진단할 수 있다.

Serous cystic neoplasm (SCN). (A) Contrast-enhanced computed tomography scan shows a well-circumscribed, honeycomb-like lesion at the body of the pancreas. (B) T2-weighted magnetic resonance image clearly shows the central scar within the cyst. (C) Gross specimen shows SCN.
3. 점액성 낭종
MCN은 난소 간질(ovarian-like stroma)을 병리 진단의 특징으로 하기 때문에 95% 이상이 여성에서 나타나고 주로 중년 여성에서 호발한다. IPMN과 마찬가지로 악성 낭종의 가능성이 있으며 조영 증강되는 벽 결절(enhancing mural nodule)이 악성을 시사하는 소견이다. 낭종의 모양은 오렌지 모양(orange-like), 다격벽(multiseptated), 낭종 내 낭종(cyst in cyst) 형태로 주로 나타난다(Fig. 4). 막(capsule)이 있으며, 드물긴 하지만 곡선형 벽 석회화(curvilinear wall calcification)가 있는 경우, 감별 진단이 용이하다. 췌관과의 교통은 없다.
Mucinous cystic neoplasm (MCN). (A) Contrast-enhanced computed tomography scan shows a round cystic mass with internal septum. (B) T2-weighted magnetic resonance image shows cyst within cyst, orange-like appearance. (C) Gross specimen shows MCN.
4. 고형 종양의 낭성 변화
때로는 고형 종괴(solid tumor)가 낭성 변화(cystic change)를 하여 낭성종양과 감별 진단을 요하는 경우가 있는데, 그 대표적인 종양이 신경내분비 종양, 선암종(ductal adenocarcinoma), 고형 가유두상 종양(solid pseudopapillary neoplasm, SPN) 등이 있다. 이 중 SPN은 출혈, 석회화를 자주 동반하고 젊은 여성에서 호발한다는 점에 감별 포인트가 있다. 신경내분비 종양의 낭성 변화는 조영 증강이 잘되는 두꺼운 벽(well-enhancing thick wall; solid component)을 동반하며, 다발성인 경우가 있다. 대부분 작은(3 cm 이하) 신경내분비 종양에서 낭성 변화가 일어나는 것으로 알려져 있으며, 예후는 비교적 좋다. 췌장암(pancreatic ductal adenocarcinoma)에서는 아주 드물게 낭성 변화를 동반하는데, 이 경우에는 대부분 저혈관성 고형병변(hypovascular solid component)을 동반하고 침윤형 성장(infiltrative growth)을 한다는 특징이 있다.
결 론
췌장낭종의 감별 진단과 그 악성도 예측에 관하여는 high-tech 영상으로 많은 진전을 이루어왔다. 가장 기본적인 검사인 복부 초음파와 CT 이외에 EUS, MRI를 적절히 사용하여 각각의 특이적인 소견을 찾을 때 그 진단능은 더욱 더 향상될 것이다.
Notes
Conflict of Interest
The author has no conflicts to disclose.