SpyGlassTM DS II와 전기수압쇄석술을 이용한 난치성 췌석의 제거
Intractable Pancreatic Stone Removal Using SpyGlassTM DS II with Electrohydraulic Lithotripsy: A Case Report and Literature Review
Article information

Abstract
췌석은 만성췌장염에서 흔히 동반되는 소견으로 반복되는 복통과 췌장염의 원인이 될 수 있다. 췌석은 췌관 협착과 자주 동반되고 췌관내 박혀 있는 경우가 많아 바스켓을 이용하여 제거하기 어렵다. 체외충격파쇄석술(ESWL)로 치료하기도 하나 반복 시술이 필요하고 성공률도 높지 않았다. 최근에 개발된 SpyGlassTM DS II (Boston Scientific, Marlborough, MA, USA)는 직경이 3.5 mm로 가늘어 췌관이 확장되어 있을 때 안으로 삽입이 가능하게 되었다. 그리고 직접 췌석을 보면서 전기수압쇄석술(EHL)이나 레이저 유도 쇄석술(laser lithotripsy)를 시행하며 췌석을 제거해 볼 수 있게 되었다. 본고에서는 SpyGlassTM DS II와 EHL을 이용하여 10 mm 이상의 다발성 췌석을 제거하는 방법을 소개하고자 한다.
Trans Abstract
Pancreatic stones are a common finding of chronic pancreatitis and may cause recurrent abdominal pain and pancreatitis. Pancreatic stones are often accompanied by stenosis of the pancreatic duct and are often impacted within the pancreatic duct, so it is not easy to remove the pancreatic stones using a basket. Until now, extracorporeal shock wave lithotripsy has been used, but it requires repeated procedures and the success rate is not very high. The recently developed SpyGlassTM DS II (Boston Scientific, Marlborough, MA, USA) has a 3.5 mm diameter that allows insertion into the dilated pancreatic duct, it is possible to remove the pancreatic stones using electrohydraulic lithotripsy (EHL) or laser lithotripsy while directly viewing the pancreatic stones. In this paper, we would like to introduce a method to remove multiple pancreatic stones larger than 10 mm using SpyGlassTM DS II with EHL.
서 론
췌석의 발생은 만성 췌장염의 흔한 합병증이며 췌석으로 인한 췌관의 압력 상승과 췌장 실질 및 췌관의 추가적 손상 때문에 췌석의 제거가 가장 효과적인 치료로 알려져 있다[1,2]. 5 mm보다 작은 췌석의 경우에는 내시경역행담췌관조영술(endoscopic retrograde cholangiography, ERCP)을 통하여 내시경 유두부 췌관괄약근 절개술(endoscopic pancreatic sphincterotomy, EPST)을 시행 후 바스켓과 풍선 카테터를 이용하여 제거할 수 있다. 5 mm보다 큰 췌석의 경우에는 쇄석술(lithotripsy)을 시행하여 제거할 수 있다. 현재 유럽소화기학회(European Society of Gastrointestinal Endoscopy, ESGE)에서는 5 mm보다 큰 췌석의 경우에 체외충격파쇄석술(extracorporeal shock wave lithotripsy, ESWL)을 1차 치료로 권유하고 있다[3]. 그러나 실제 임상에서는 ESWL을 이용한 췌석 파쇄는 경우에 따라서 그 효과를 보기 어려운 경우가 많이 있다. 본고에서는 ESWL을 통한 췌석 파쇄는 실패하였지만 SpyGlassTM DS II (Boston Scientific, Marlborough, MA, USA)로 직시하에 전기수압 쇄석술(electrohydraulic lithotripsy, EHL)을 이용하여 췌석 제거에 성공하였던 증례를 소개하고자 한다.
증 례
74세 남자 환자가 외부 복부 초음파에서 여러 개의 담낭 결석과 췌관이 4.8 mm까지 확장된 소견으로 의뢰되었다. 이와 관련된 복부 통증 외에는 호소하는 다른 증상은 없었다. 환자는 수 년 전에 담도 결석을 제거하였으며 최근에 당뇨를 진단받았다. 30갑년의 흡연력이 있으며 소주 반 병 정도를 주 2-3회 마시는 음주력이 있었다. 내원 당시 혈액 검사에서 당화혈색소가 8.6%로 상승되어 있는 것 외에 이상 소견은 보이지 않았다. 복부 전산화단층촬영에서 췌장 두부에 다발성 췌석과 함께 주췌관이 미만성으로 확장되어 있었으며, 두부 쪽에는 6 mm 안팎으로 미부에는 5 mm 안팎으로 췌관이 확장되어 있었다. 췌장 실질은 위축 소견을 보이고 있어 만성 췌장염에 합당하였다(Fig. 1). 담낭에는 담낭 선근종증과 함께 작은 다발성 담낭결석이 관찰되었다. 췌관 배액술(endoscopic retrograde pancreatic drainage)을 플라스틱 배액관(Geenen® Pancreatic stent, GPSO 7 Fr., 7 cm, COOK Medical, Limerick, Ireland)으로 시행하였고 이후 복강경 담낭절제술을 진행 하였다. 경과는 양호하여 3개월마다 췌관 배액관(Zimmon® Pancreatic stent, SPSOF 7 Fr., 9 cm, COOK Medical)으로 총 3회 교체하였다. 그리고 ESWL을 Sonolith i-move (EDAP TMS, Rhône, France)를 이용하여 3회 시행하였으나 췌석 파쇄는 실패하였다. SpyGlassTM DS II 직시하에 EHL을 이용하여 췌석을 파쇄하기로 계획하였다. ERCP를 시행하여 췌관에 도구 삽입 및 췌석 제거를 용이하게 하기 위해 Fusion® Titan balloon (COOK Medical Inc., Winston-Salem, NC, USA)을 6 mm까지 30초간 시행하여 근위부 췌관 확장술을 먼저 하였다. 그리고 SpyGlassTM DS II를 삽입하여 췌석을 정확하게 조준하여 EHL을 시행할 수 있었다. EHL은 WA09408A, P3/3m/f (Walz Elecktronik, Rohrdorf, Germany) 프로브를 이용하여 250 mJ 강도에서 시작하였으나 췌석 파쇄가 원활하지 않아 500 mJ까지 강도를 증가시켜서 시행하였다. 췌장 두부와 체부의 1 cm 이상의 췌석 뿐만 아니라 췌장 꼬리부분 쪽의 췌석들도 정확하게 조준하여 분쇄할 수 있었다(Fig. 2). 이렇게 분쇄된 췌석들은 바스켓(Olympus Flower-basket, 8 wire type, 7 Fr., 0.035 inch, Tokyo, Japan)과 풍선 카테터(15 mm balloon, COOK Medical Inc.)를 이용하여 제거하였다(Fig. 3). 시술은 이틀에 걸쳐서 총 2회 시행하였으며 모든 췌석을 성공적으로 제거하였다.
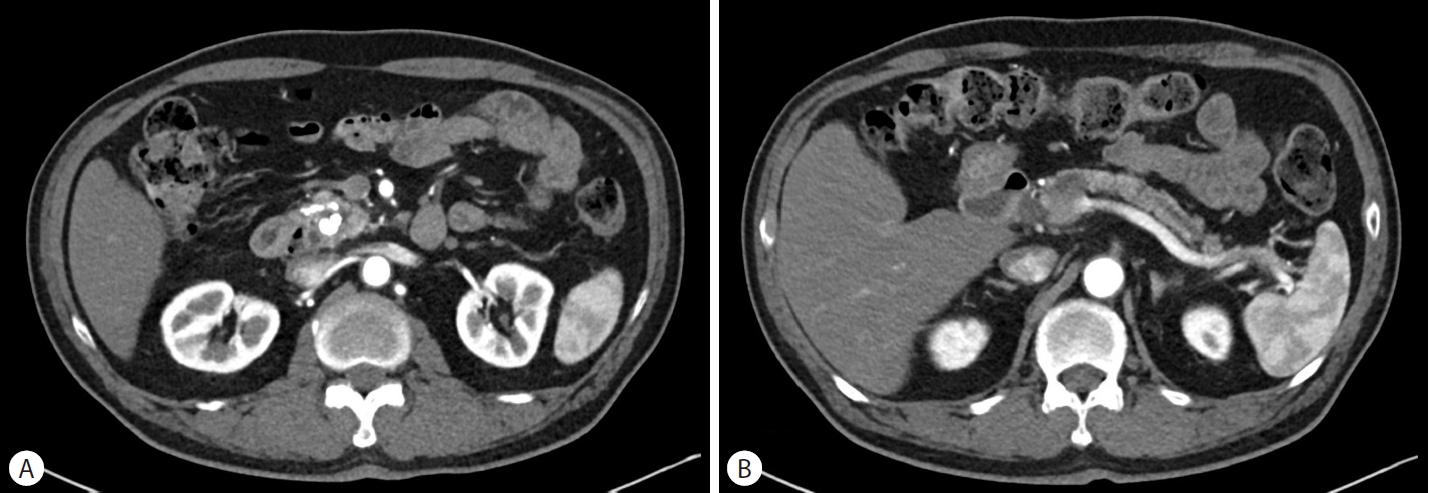
intital CT images on diagnosis. (A) Multiple stones in pancreas head. (B) dilated main pancreatic duct.
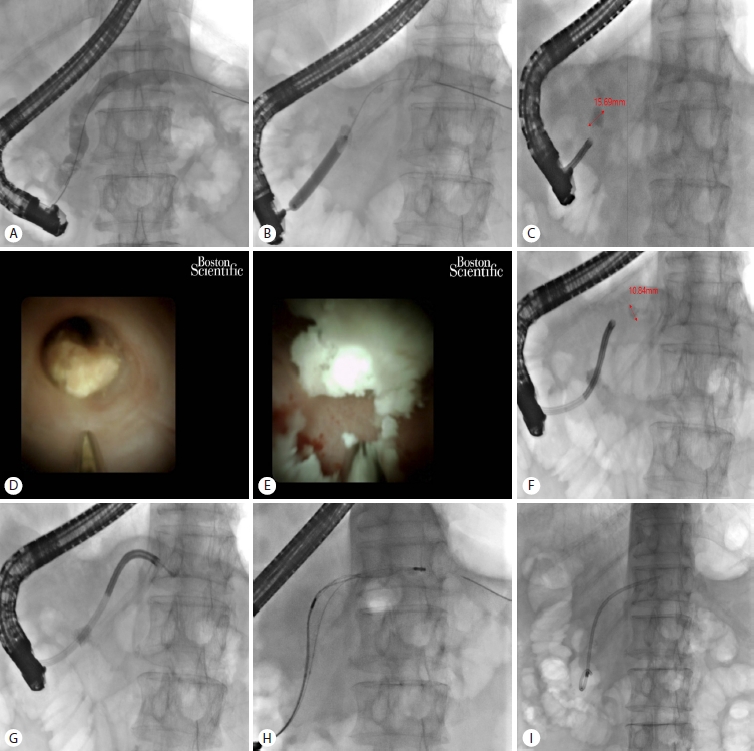
These figures present the sequence of pancreatic stone removal by using SpyglassTM dS Ⅱ with electrohydraulic lithotripsy (ehL). (A) initial pancreatogram shows dilatated the main pancreatic duct duct with multiple pancreatic stone. (B) Proximal pancreatic duct dilatation was done by fusion® Titan balloon upto 6 mm for 30 seconds. (C) A stone in pancreas head larger than 1.5 cm. (d) Spyglass image shows pancreas stone that is targeted by ehL. (e) This Spyglass image shows pancreatic stone being destroyed by ehL. (f) Stone in the pancreas body larger than 1 cm. (g) Small stone in pancreas tail. (h) Stones retrieved by using basket. (i) The stones removed and endoscopic retrograde pancreatic drainage stent was placed.
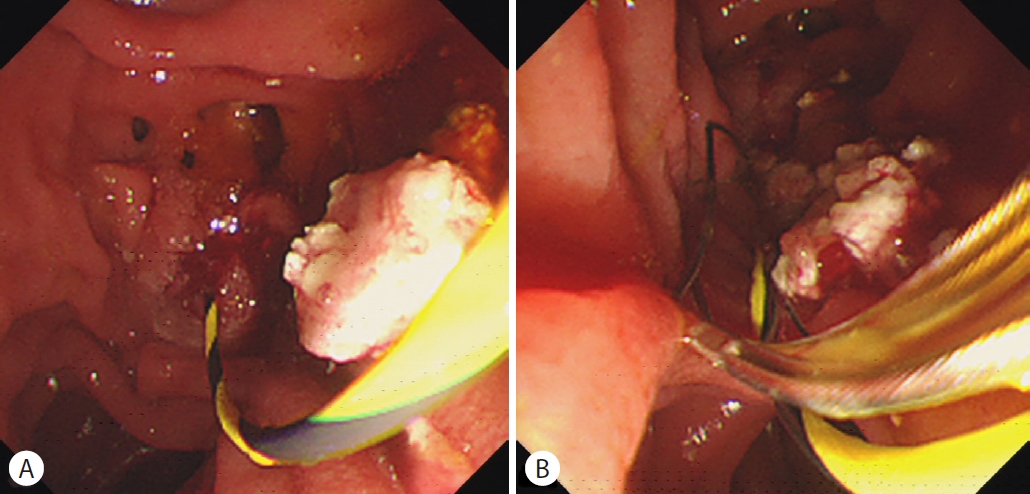
(A) Large stone was removed from pancreas head by 4 wire dormia basket. (B) fragmented stone were extracted from pancreas body by 8 wire flower basket.
고 찰
만성 췌장염에서 췌석을 내시경으로만 제거하기는 쉽지 않다. 5 mm 이하의 췌석은 EPST를 통해서 제거 가능하지만, 특히 크기가 10 mm 이상이거나 췌관에 협착이 있을 경우에 내시경적 제거는 실패하기 쉽다. 이를 극복하기 위해서 ESWL이 도입이 되었고, ESWL을 이용해서 췌석을 분쇄해서 안전하고 효과적으로 제거할 수 있게 되었다. ESGE 진료지침에서도 5 mm 이상의 췌석에 대해서 ESWL 시행을 우선 고려해보기를 권하고 있다[3]. 만성 췌장염에서 ESWL을 이용한 췌석 제거에 대해서 최근 메타분석(meta-analysis)을 보면 완전제거율(complete ductal clearance)은 69.8%였고 통증의 감소는 64.2%에서 있었으며, 이는 과거 연구들과 비슷한 결과를 보여주고 있다[4]. 하지만 췌관에 다병소 협착(multifocal stricture)이 있거나 췌장 미부에 췌석이 있는 경우에는 ESWL을 이용해서도 제거하기가 어렵다[5].
ESWL 외에도 췌관 결석을 파쇄하고 제거하는 기술로는 기계적 쇄석술(mechanical lithotripsy), EHL 그리고 레이저 유도 쇄석술(laser lithotripsy) 같은 기술들이 있다. 하지만 기계적 쇄석술에 있어서 담도와 달리 췌관은 직경이 넓지 않아 바스켓을 통한 췌석 포획이 어렵다. 또한, 유용한 쇄석용 바스켓도 개발되어 있지 않아 거의 사용되지 않으며, EHL과 레이저 유도 쇄석술은 연구된 데이터가 제한적이다[6].
SpyGlass 시스템은 일회용 디지털 담췌관용 내시경으로 2009년 미국 Food and Drug Administration (FDA)에 췌담도 질환의 진단과 치료의 내시경적 시술에 승인되었고, 육안으로 병변을 직접 보면서 정확하게 확인하며 검사와 치료를 진행할 수 있어 장점이 많다[7,8].
Ito 등[9]의 연구에서 98명의 환자에서 81.6%에서 췌석을 제거에 성공하였으며, 이 중 7.1%에 해당하는 환자들은 SpyGlass 시스템 혹은 엑스선 검사 하에 췌석을 제거했다. 이 연구에서 1차적으로 ESWL로 췌석 분쇄에 실패한 경우에 주췌관 협착에도 불구하고 유도철사의 조작이 용이하다면 EHL을 SpyGlass 혹은 엑스선 검사 하에 성공적으로 췌석 제거가 가능함을 보여주고 있다[9]. 또한 Bekkali 등[10]에서 SpyGlass DS와 함께 EHL을 이용하여 췌석 제거에 대한 후향적 연구를 보고하였다. 환자 수가 적긴 하지만 83% (5/6)에서 췌석 파쇄와 췌관 감압에 성공하였다고 보고했으며, 난치성 췌석 제거에 SpyGlass 직시하에 EHL이 좋은 기술이 될 수 있다고 결론 짓고 있다[10].
본 환자의 경우에도 췌관의 다병소 협착과 췌장 두부 뿐만 아니라 체부와 미부에도 1 cm 이상의 췌석들이 있었으나 SpyGlass 관찰 하에 EHL을 시행하여 성공적으로 모두 제거할 수 있었다. 향후에 이와 같은 난치성 췌석에 대하여 SpyGlassTM DS II 직시하에 EHL로 치료한 데이터가 축적되어 안정성이 확보된다면 훌륭한 췌석 제거의 도구가 될 것으로 판단된다.
Notes
Conflict of Interest
The authors have no conflicts to disclose.