위절제 후 루와이 소장 재건술을 받은 환자의 내시경역행담췌관조영술에서 단축형 단일풍선 소장내시경을 이용한 Mechanistic Loop Resolution Strategy의 유용성
Mechanistic Loop Resolution Strategy for Short-Type Single-Balloon Enteroscopy-Assisted Endoscopic Retrograde Cholangiopancreatography in Roux-en-Y Reconstruction
Article information

본 고에서는 위암 수술 후 위절제와 루와이(Roux-en-Y) 소장 재건술을 받은 환자에서 단축형 단일풍선 소장내시경의 일반적인 접근 과정과 난치성 루프형성의 형태를 분석한 Yang 등의 연구1를 소개하고 임상적 유용성과 제한점에 대해 논의해보고자 한다.
수술 후 상부위장관의 해부학적 변이가 동반되어 통상적인 내시경으로 주유두부까지 도달이 어려운 환자에서 단축형 풍선 소장내시경이 점차 표준 내시경역행담췌관조영술(endoscopic retrograde cholangiopancreatography, ERCP) 술식으로 자리잡아 가고 있다. 그러나 루와이 소장 재건술의 경우에는 상대적으로 긴 길이의 소장, 소장의 유동성(redundancy), 장간막과 소장의 유착, 공장-공장 문합 부위의 유착과 예각 형성 등으로 인해 다른 해부학적 변이에 비해 ERCP 시술 성공률이 낮았고, 대부분의 실패는 내시경 접근의 어려움에 기인하였다. 저자들은 이러한 결과가 루와이 구조에 대한 내시경 접근 과정이 표준화되지 못하고, 경험 많은 시술자의 임기응변적 대응에 의존해 왔기 때문에 시술의 재현성이 떨어지는 것으로 판단하였다. 이에 본 연구에서는 일차적으로 위암 수술 후 위절제와 루와이 소장 재건술을 받은 환자에서 단축형 단일풍선 소장내시경의 일반적인 접근 과정을 저자들의 경험에 기반하여 도식화하고자 하였다. 이에 더하여 접근 과정에서 실패의 주 원인이 되는 난치성 루프형성의 형태를 분석하고 이를 해결하기 위한 대안적 방안을 제시하고자 하였다. 그리고 이들을 통합하여 “mechanistic loop resolution strategy”라는 표준화된 접근 방식을 도출하고자 하였고, 이 방식의 재현성과 안전성을 평가하였다.
위절제 후 루와이 재건술을 받은 환자에서 표준화된 단일 풍선 소장 내시경 접근 방법은 Fig. 1에 도식화하여 제시하였다. 난치성 루프의 대표적인 형태는 지팡이 모양의 cane-shape 루프 형성(Fig. 1G)이다. 가장 단순한 방법은 외측튜브를 최대한 지팡이의 손잡이 가까이까지 위치시킨 후 , 지팡이의 몸통(shaft)을 지지하면서 내시경을 단순하게 미는 방법이다. 이것이 여의치 않을 때는 Fig. 2B-D에서 보이는 것처럼 지팡이 손잡이 부분을 180도 뒤를 향하도록 돌린 다음, 지팡이의 손잡이와 몸통의 주행 방향이 알파루프가 되도록 인위적으로 소장의 주행을 변경한다. 이 알파루프의 힘을 받아서 일단 내시경을 넘긴 후 차후 알파루프를 풀어주는 방법(Fig. 2H, I)이다.
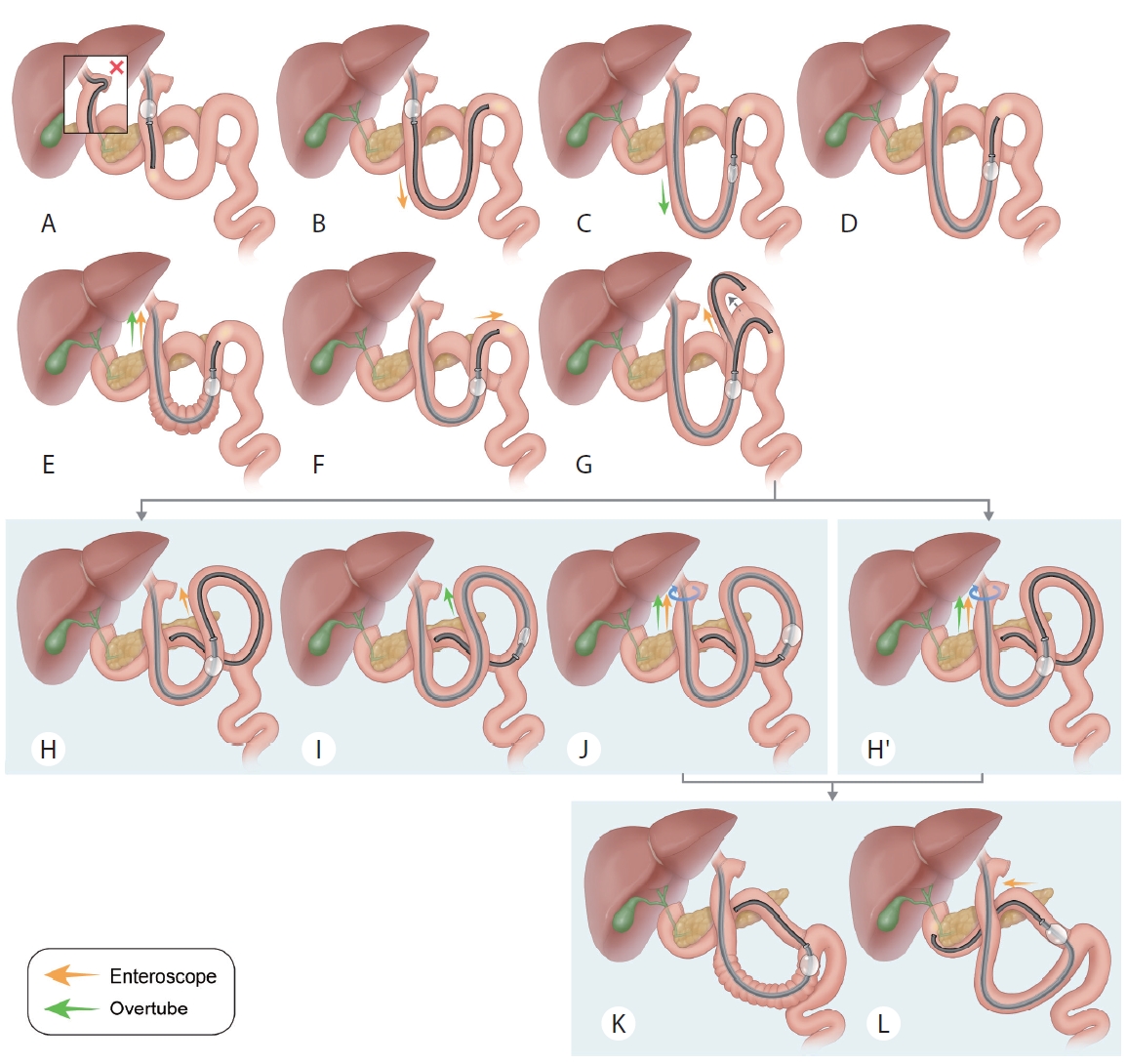
Mechanistic loop resolution strategy for gastrectomy with Roux-en-Y reconstruction.
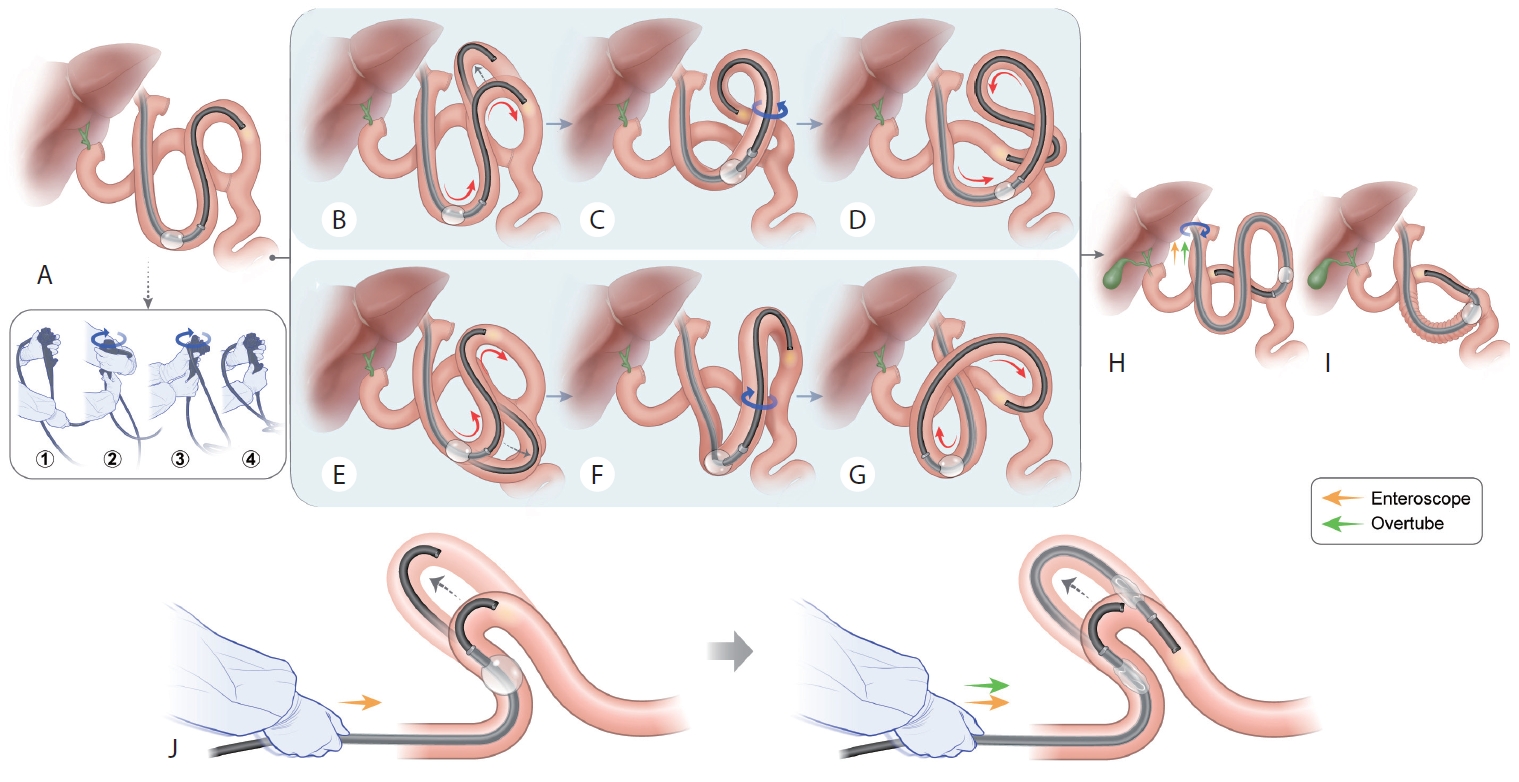
Mechanistic loop resolution strategy for difficult cane or S-shaped loop. (A-I) Conversion of the bowel loop pattern from the cane or S-shaped loop to three-dimensionally rotated loops with ring structures using the extreme rotational maneuver. (J) Forceful pushing through maneuver by simultaneously holding the enteroscope and overtube together.
가장 어려운 난치성 루프는 cane-shape 루프와 비슷하면서도 약간 다른 S-shape 루프이다(Fig. 3). S-shape 루프에서는 cane-shape 루프와 다르게 내시경을 밀었을 때 S자의 머리 부분이 아니라 배부분이 더 불룩해지면서 내시경이 전진하지 않는다. 따라서 S자의 배부분을 인위적으로 돌려서 여기에 알파루프를 만들어 주어야 한다(Fig. 2E-G). 이후 어려운 위치를 넘긴 후 알파루프를 다시 풀어준다(Fig. 2H, I). Cane-shape과 S-shape 루프를 극복하는 공통적인 원리는 cane이나 S의 머리 부분과 몸통의 vector 방향이 상호 불일치하는 상황(Fig. 3)을 인위적인 변경을 통해 비슷한 방향의 vector로 변형해 주는 것이다. 이를 위해 cane이나 S-shape 루프의 머리와 몸통이, 3차원 고리형 루프인 알파루프를 이루도록 만들어 주어야 한다. 이를 위해서는 내시경의 주행을 인위적으로 바꿔주는 과정이 필요한데 저자들은 Fig. 2의 하단의 ①-④에서 보여지는 것 같이 내시경의 control section을 인위적으로 돌려서 내시경을 extreme rotation시키는 방법으로 이를 시행하고 있다. 모든 방법이 여의치 않을 때는 외측튜브의 풍선을 탈기한 상태에서 외측튜브와 내시경을 함께 잡고 동시에 pushing을 하는 방법(Fig. 2J)도 사용하고 있다.

Mechanism of the paradoxical phenomenon related to S-shaped loops (S, reverse S, or recumbent S).
저자들은 Fig. 1과 Fig. 2의 방식을 통합하여 mechanistic loop resolution strategy라고 명명하고 2년 동안 위암 수술 후 루와이 재건을 받은 37명의 환자에서 총 43회의 ERCP를 시행하였고 모든 케이스에서 내시경 도달에 성공하였고 1st session에서 ERCP 성공률은 87.8%, 2nd session까지 고려한 ERCP 성공률은 92.7%를 기록하였으며 삽입 과정에서 천공은 발생하지 않았다(Table 1).
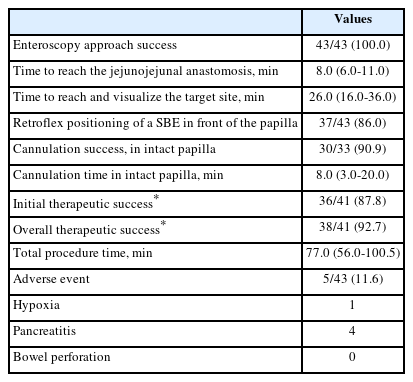
ERCP outcomes and adverse events
논 평
Yang 등[1]이 발표한 위절제와 루와이 소장 재건술을 받은 환자에서의 ERCP를 위한 단축형 단일풍선 소장내시경을 이용한 접근법에 대한 연구는 루와이 구조에 대한 내시경 접근 과정을 표준화하고 나아가 숙련된 내시경의사뿐만 아니라 초심자도 시술을 진행하는 데 있어 효율적인 삽입을 도모하고 천공 등과 같은 합병증을 예방하는데 매우 의미 있는 연구이다. 본 고에서는 논문의 임상적 의미와 제한점에 대하여 기술하고자 한다.
수술 후 변형된 구조에서의 ERCP는 본 연구에서 제시하는 난치성 루프를 해결하기 위한 다양한 술기들 이외에도, 수입각(afferent loop)을 선별하는 과정이 매우 중요하다. 공장 문합부에서 두 개 혹은 세 개의 경로 중 어떤 경로로 진입해야 담관에 도달할 수 있는지를 빠르고 정확하게 판단할 수 있다면 불필요한 삽입과정을 생략할 수 있고 그로 인한 내시경 삽입 관련 합병증을 최소화할 수 있다. Tsutsumi 등[2]은 공장 문합부의 문합 형태에 따라 크게 측 - 단 공장문합(side-to-end jejunojejunostomy, SE-JJ)와 측-측 공장문합(side-to-side jejunojejunostomy, SS-JJ) 두 가지로 분류를 소개하였다. 이러한 분류에 따르면 내시경이 공장 문합부에 도달하였을 때 SE-JJ의 경우 매우 긴 두 개의 진입각을 관찰할 수 있고, 이때 임의로 어느 한 진입각으로 내시경을 삽입하는 경우에는 잘못 진입하였을 때 공장 문합부까지 회수하여 다시 다른 진입각으로 재진입을 하는 과정이 필요하다. 반면 SS-JJ의 경우는 세 개의 진입각 중 가장 가운데 있는 진입각이 담관에 도달할 수 있는 수입각일 가능성이 높다(Fig. 4). 이러한 분류에 기반하여 저자들은 59명의 SE-JJ를 시행받은 환자들 중 84%에서 담관에 도달하였던 반면 31명의 SS-JJ를 시행받은 환자들 중 100%에서 담관에 도달하였다고 보고하여 SS-JJ가 SE-JJ에 비하여 수입각을 쉽게 감별할 수 있고 보다 쉽고 확실하게 담관에 도달할 수 있다.

Type of jejunojejunostomy in Roux-en-Y reconstruction. (A) Schema of the operation procedure of side-to-end jejunojejunostomy; endoscopic view encountering two-pronged lumens at the jejunojejunostomy; fluoroscopic image showing the short-type double-balloon enteroscope in the afferent loop. (B) Schema of the operation procedure of side-to-side jejunojejunostomy; endoscopic view encountering three-pronged lumens at the jejunojejunostomy; fluoroscopic image showing the cap-assisted colonoscope in the afferent loop.
이와 유사한 Lee 등[3]의 연구에서는 루와이 재건술을 받은 환자에서 풍선 보조소장 내시경의 도움 없이 대장내시경으로 ERCP를 시행하였고, SS-JJ의 진입 성공률은 SE-JJ군에 비하여 통계학적으로 유의하게 높았다(34/38 [89.5%] vs. 1/9 [11.1%], p <0.001). 또한 다변량 로지스틱 분석에서 내시경 진입 성공과 관련 있는 인자는 SS-JJ 문합 형태가 유일하였고, 실제 내시경 진입이 매우 어렵다고 알려진 위 보존 유무는 성공율에 별다른 영향을 끼치지 않았다.
본 논문은 아쉽게도 위절제를 하지 않고 루와이 소장 재건술을 시행한 루와이 간공장 문합술 환자 등은 포함하지 않았다. 이러한 수술 후 변형은 보존되어 있는 위의 대만부에 형성되는 루프로 인해 매우 접근이 어려운 해부학적 변이이다. 이 경우에도 Yang 등이 제시한 다양한 접근 방법이 공통적으로 이용되기는 하지만, 이에 더하여 위의 대만부의 루프, 상/하 십이지장각과 십이지장-공장 이행부에 걸쳐서 형성되는 S-shape 루프에 대한 추가적인 대처가 필요할 수 있다. 현재 저자들은 이 해부학적 구조를 극복하기 위한 mechanical loop resolution strategy를 연구 중이고 가설 수립과 도식화 과정을 진행하고 재현성(reproducibility)에 대한 내부 평가를 계획 중으로 알고 있어, 근 시일 내에 발표될 후속 논문이 매우 기대가 된다. 또한 추가적으로 SE-JJ에 대한 루와이 구조 이외에도 복잡하고 다양한 구조의 SS-JJ (e.g. modified Child surgery)에 대한 표준화 작업도 필요할 것으로 생각된다. 차후 보고된 후속 연구들을 통해 다양한 해부학적 구조의 ERCP에 대한 표준화가 이루어질 수 있기를 기대한다.
Notes
Conflict of Interest
Min Jae Yang is currently serving as an Editor in the Editorial Board of the Korean Journal of Pancreas and Biliary Tract; however, Min Jae Yang was not involved in the peer reviewer selection, evaluation, or decision process of this manuscript.
Acknowledgements
This work was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government (NRF-2021R1C1C1008619).