관내 유두상 점액성 종양의 병리학적 고찰
Pathologic View of Intraductal Papillary Mucinous Neoplasm
Article information

Abstract
최근에 영상 기술의 발전으로 췌장의 관내 유두상 점액성 종양(Intraductal Papillary Mucinous Neoplasm, IPMN)이 자주 관찰된다. IPMN은 병리학적으로 췌관의 확장과 동반하여 종양성 점액세포의 관내 증식과 유두 형성을 특징으로 하는 질환이다 . 종양의 침범 위치에 따라 주췌관형(main duct-IPMN)과 분지관형(branch duct-IPMN), 그리고 혼합형(mixed type)으로 분류한다. 또 종양세포의 조직학적 특성에 따라 저등급 이형성(low grade dysplasia)과 고등급 이형성(high grade dysplasia)으로 분류하며, 종양세포의 형태에 따라 위, 장, 췌담도 및 호산성 아형으로 분류한다. 최근에는 내시경초음파 세포검사 뿐만 아니라 암배아항원이나 아밀라아제의 화학적 분석이나 GNAS 돌연변이와 같은 분자병리검사가 진단에 도움이 된다.
Trans Abstract
Among pancreatic cystic lesions, mucinous cystic neoplasm (MCN) and intraductal papillary mucinous neoplasm (IPMN) of the pancreas are precursor lesions of pancreatic adenocarcinoma. IPMN is characterized by intraductal papillary proliferation of mucin-producing epithelial cells that exhibit various degrees of dysplasia. IPMN is classified as the main duct type (MD-IPMN), mixed type and the branch duct type (BD-IPMN) according to the location of involvement, and into four histological subtypes (gastric, intestinal, pancreatobiliary, and oncocytic) according to the histomorphological and immunohistochemical characteristics. Most patients with MD-IPMN undergo tumor resection due to moderate to high risk of malignancy. Patients with BD-IPMN who do not undergo resection may develop malignant change, and concomitant separate pancreatic cancer occurs in 2-10% of patients with IPMN. Patients with BD-IPMN who do not undergo resection should do careful surveillance including endoscopic ultrasound sonography for the early detection of malignant change and separate pancreatic cancer.
서 론
췌장은 다양한 낭성 변화를 동반하는데 최근에서 영상 기술이 발전하면서 췌장의 낭성 병변이 더욱 자주 관찰된다[1]. 췌장의 낭종은 비종양성 낭포와 종양성 낭종으로 나눌 수 있다. 비종양성 낭포는 가낭포(pseudocyst)와 염증과 연관하여 발생하는 낭포 등을 말한다. 종양성 낭종은 다양한 세포 기원의 종양에서 낭성 변화를 보이는 것을 의미하는 것으로, 전체 낭성 병변의 60% 정도를 차지한다.1 종양성 낭성 병변의 대부분은 관 구조 기원의 종양으로 종양 세포의 특징에 따라 점액성 또는 장액성 낭성 종양 등으로 나눈다. 췌장의 점액성 종양성 낭종 중 관내 유두상 점액성 종양(Intraductal Papillary Mucinous Neoplasm, IPMN)은 모든 절제된 췌장의 20-30%에 달하는 종양으로 최근에 발생 빈도가 더욱 증가하고 있다[2]. 이에 IPMN의 특징을 병리학적 관점에서 살펴보고자 한다.
본 론
1. IPMN의 특징
췌장에서 발생하는 이질적인 낭성 병변은 1990년대에 처음 보고되었고, IPMN이라는 용어는 World Health Organization(WHO)의 2000년 분류에서 정립되었다[3]. IPMN은 병리학적으로 일반적으로 유두를 형성하고 췌관의 낭포성 확장과 임상 및 육안으로 감지할 수 있는 종괴를 형성하는 종양성 점액 세포의 관내 증식을 특징으로 한다(Fig. 1). 진단 시 평균 연령은 68세로 여성보다 남성에서 약간 더 자주 관찰되며 주로 췌장의 두부에서 발생한다[1,4]. 두꺼운 점액이 생성되는 것이 특징이며 주췌관과 분지관의 확장과 점액 분비 췌관 상피의 관내 증식 그리고 주변 췌장의 위축을 동반한다. 2012년과 2017년의 Fukuoka 지침에 따르면 췌관 폐쇄의 뚜렷한 원인없이 직경 5 mm 이상의 가시적인 주췌관 확장 병변을 가지는 종양을 이르며 이는 췌관과 연결되어 있다[5,6].

Histologic features of intrapapillary mucinous neoplasm (IPMN). (A) IPMN with low grade dysplasia. (B) IPMN with high grade dysplasia. (C) IPMN with invasive ductal adenocarcinoma (A, B: H&E, ×200, C: H&E, ×100).
반면에 점액성 낭성 종양(Mucinous Cystic Neoplasm, MCN)은 IPMN과 마찬가지로 췌장에서 점액을 분비하는 종양의 하나로 진단 시 평균 연령은 48세로 95% 이상 폐경기 전후의 여성에서 발생하며, 종양의 95% 정도가 췌장의 체부와 미부에서 발견된다[4,6,7]. 육안상으로 췌관과는 연결이 없고 특히 조직학적으로 점막 상피 주위에 난소 기질을 가지는 특징이 있다. IPMN과 MCN은 췌장암종의 전구 병변으로 알려져 있다[8,9].
낭포액에서 암배아항원(Carcinoembryonic Antigen, CEA)을 분석하면 점액성 췌장 낭성 종양에서 비점액성 종양에 비해 특이하게 증가한다[10]. 따라서 IPMN과 MCN에서 점액성 낭포액을 분석하면 두 종양 모두에서 동일하게 CEA 증가와 RNF43 돌연변이를 관찰할 수 있다[6,11]. KRAS 유전자의 코돈 12의 점 돌연변이는 췌장의 선암종(67%)에서 다수 관찰되었으나 IPMN이나 만성 췌장염에서도 관찰되어 이것으로 암종과 선종의 감별은 어렵다[12]. 최근에 IPMN의 41-75%에서 코돈 201에서 활성화된 GNAS 돌연변이를 발견하여 이는 IPMN 진단에 매우 특이적인 유전적 변형으로 알려져 있다[12].
2. IPMN의 분류와 진단
비침습적 IPMN은 조직학적 특징에 따라 저등급 이형성(low grade dysplasia)과 고등급 이형성(high grade dysplasia)으로 나눈다(Fig. 1) [8]. 조직학적으로 유사분열이나 괴사없이 방향이 좋고 작고 균일한 핵을 가진 단일 층의 종양 세포를 갖는 것은 저등급 이형성 IPMN으로 분류한다. 핵 다향성을 동반하고 여러 층으로 중첩되거나 채모양으로 붙어있는 등 심각한 행의 극성 상실과 유사분열이 종종 관찰되는 병변은 고등급 이형성 IPMN으로 분류한다.
IPMN은 조직학적 형태에 따라 4가지 조직학적 아형(위, 장, 췌담도 및 호산성)으로 분류한다(Fig. 2) [13]. IPMN은 위 아형이 제일 많고, 면역조직화학염색에서 MUC5AC와 MUC6에 양성을 나타낸다. IPMN의 장 아형은 MUC2와 MUC5AC에 양성, 췌담도 아형은 MUC1과 MUC5AC에 양성, 그리고 호산성 아형은 MUC1과 MUC6에 양성으로 구별할 수 있다 [14]. IPMN의 장, 췌담도 및 호산성 아형은 주로 주췌관에서 발생하지만 위 아형은 일반적으로 분지관에서 발생한다[8,13,14].

Histologic subtypes of tumor cells lined along the cystic lesions of intrapapillary mucinous neoplasm (IPMN). (A) Gastric subtype. (B) Intestinal subtype. (C) Pancreatobiliary subtype (A, B: H&E, ×200, C: H&E, ×400).
IPMN은 종양 침범 위치에 따라 주췌관형(Main Duct IPMN, MD-IPMN)과 분지관형(Branch Duct IPMN, BD-IPMN), 그리고 혼합형(mixed type)으로 분류한다[6]. MD-IPMN은 전체 IPMN 중 24.7% 정도로 췌장의 주췌관 확장 소견을 보이고 종양 주위에 만성 췌장염을 동반한다[5]. MD-IPMN은 약 62.2% 정도에서 침윤성 암종으로 이행한다[4,5,15]. 반면, BD-IPMN은 56.8% 정도의 빈도로 분지관에 국한되어 발생하고 비교적 젊은 연령에서 발생하며, 약 10-22% 정도 침윤성 암종으로 이행한다[4,5,16]. 주췌관형과 분지관형을 모두 가지고 있는 혼합형의 경우는 17.6% 정도 빈도로 발생하며 57.6% 정도에서 침윤성 암종으로 이행한다(Fig. 1) [5]. IPMN이 침습적이 되면 일반적으로 관형 및 콜로이드 암종이라는 두 가지 다른 유형의 침습성 암종이 발생한다(Fig. 1) [13,17].
내시경초음파 세포검사로 IPMN을 진단할 수 있는데 이 때 점액의 배경에 다양한 이형성 정도의 점액 상피의 유두 조각을 관찰할 수 있다(Fig. 3). IPMN은 핵 이형성, 현저한 핵소체, 핵 불규칙성 및 세포 밀집으로 나타나는 고등급 이형성에 대해 잘 평가해야 한다[1].
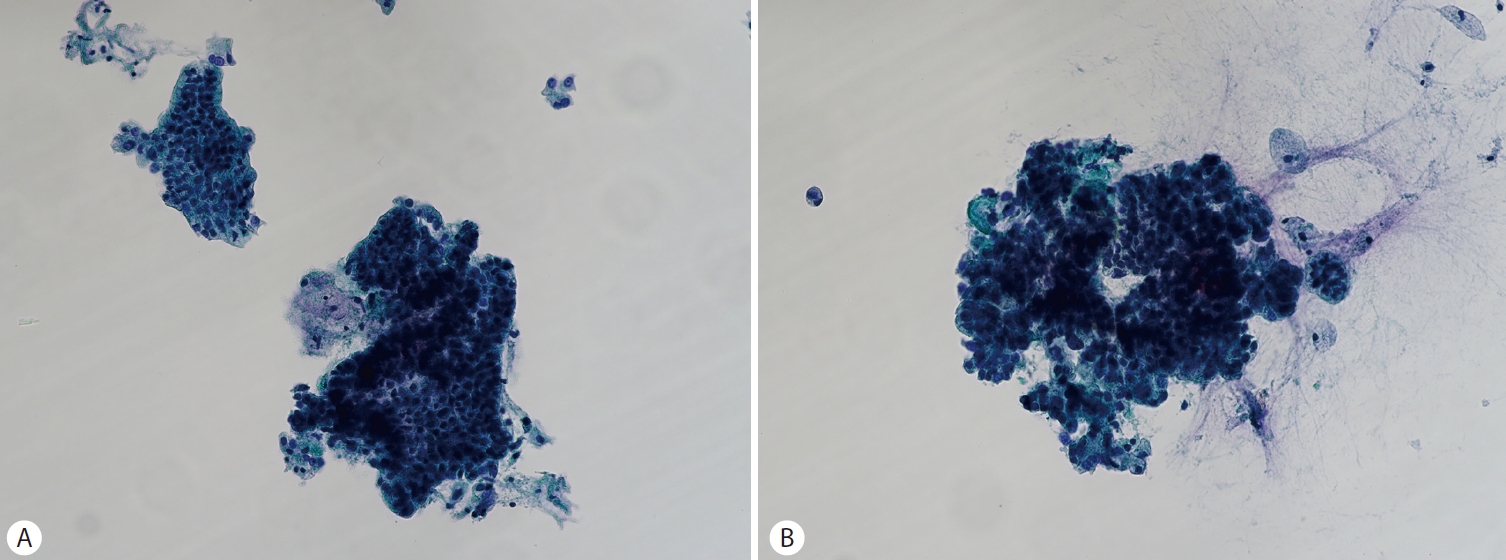
Endoscopic ultrasound-guided fine needle aspiration cytology of intrapapillary mucinous neoplasm (IPMN). (A) A few papillary cell clusters with variable degree of dysplasia. (B) A tight papillary epithelial cluster with nuclear atypia, prominent nucleoli, nuclear irregularity and cell crowding (A, B: Papanicolaou stain, ×200).
내시경초음파 세포검사로 얻은 낭포 내용물의 세포뿐만 아니라 암배아항원(>200 ng/mL) 분석은 점액성 췌장 낭성 병변을 구별하는데 쓰이고 아밀라아제(<250 IU/L) 분석은 가성낭종을 배제하는데 종종 유용하다[10,18]. 그러나 이들 내시경초음파 세포검사로 얻은 낭포 내용물의 세포학이나 암배아항원, 아밀라아제 화학적 분석으로는 MCN과 IPMN을 구별할 수 없다[10]. 따라서 임상 병력, 성별, 영상 특성, 세포학, 낭포액, 암배아 항원 및 아밀라아제의 화학적 분석 그리고 KRAS나 GNAS 등 분자검사들을 조합하여 비로소 췌장의 낭종을 점액성 또는 비점액성으로 특징지을 수 있을 뿐만 아니라 특정 하위 유형을 보다 정확하게 감별할 수 있다[1,12,19-21].
3. 관내 유두상 점액성 종양의 치료와 예후
2017년 IPMN 관리 지침에 따르면 '고위험군(high-risk stigmata)’ (췌두부 낭성변화를 가진 환자의 폐쇄성 황달, 조영 증강된 5 mm 이상의 결절, 10 mm 이상의 주췌관 크기)이 있는 환자는 절제술을 받아야 한다고 권장한다[6]. 또 ‘우려되는 특징(worrisome features)’ (3 cm 이상 크기의 낭종, 조영 증강된 5 mm 미만의 결절, 두껍게 조영 증강된 낭종 벽, 5-9 mm의 주췌관 크기, 말단 췌장 위축을 동반한 주췌관 구경의 급격한 변화, 림프절병증, CA19-9 혈청 수치 상승 및 2년에 5 mm 이상의 빠른 낭종 성장)은 내시경 초음파에 의해 평가되어야 한다[6].
종양의 위치와 세포 형태에 따라 대부분의 MD-IPMN 환자는 종양 절제술을 받아야 한다[22]. 절제술을 받지 않은 BD-IPMN 환자는 악성 변화의 조기 발견과 별도의 췌장암을 위해 내시경 초음파를 포함한 세심한 감시를 받아야 한다[23]. 고등급 이형성 또는 침윤성 암종을 동반하였거나 장 또는 췌담도 아형의 IPMN 환자는 초기 절제 후 잔여 췌장에 대한 면밀하고 장기적인 감시를 받아야 한다. IPMN은 췌장 선암종에 비해 양호한 예후를 나타내지만, IPMN에 대한 부분 췌장 절제술 후, 잔존 췌장에서 고위험 병변의 이차적 발생 위험에 대한 평가는 수술 후 감시 방식 및 추적 기간을 확립하는 데 중요하다[24].
결 론
췌장 낭성 종양 중 IPMN과 MCN은 췌장 선암종의 전구 병변이다[4,8]. 따라서 육안적으로 종양의 위치와 크기 기술을 정확하게 하고 조직학적으로 이형성 정도에 따라 저등급, 고등급으로 분류하고, 침윤성 선암종의 존재 여부를 세심하게 잘 살펴 진단하는 것이 중요하다. 또한, 내시경초음파 세포 검사로 얻어진 세포 검체를 세포학적 특징에 따라 정확하게 진단하거나 분자병리학적 분석을 통해 유전자 변이 유무를 파악하는 것이 진단에 도움이 될 것이다[2]. 그 외에도 관내 상피의 아형 분류나 면역조직화학 검사 및 림프절 전이 유무 기술 등으로 예후 예측에 도움이 될 수 있다.
Notes
Conflicts of Interest
The authors have no conflicts to disclose.