INTRODUCTION
Most brain metastases arise from three major malignancies: lung cancer, breast cancer, and malignant melanoma [1]. Brain metastases originating from gastrointestinal cancer are extremely rare. The incidence of brain metastasis from gastric cancer is below 1% and that from colorectal cancer is approximately 4% [2-4]. Metastases to the brain and central nervous system are very rare from pancreatic cancer; only about 0.33% of pancreatic cancers metastasize to the brain [5].
In this report, we present a case of resected pancreatic cancer with brain metastasis after long-term remission. We also systematically reviewed published articles on brain metastases originating from pancreatic cancer, which focused on patient characteristics, clinical appearance, management, and outcomes.
CASE
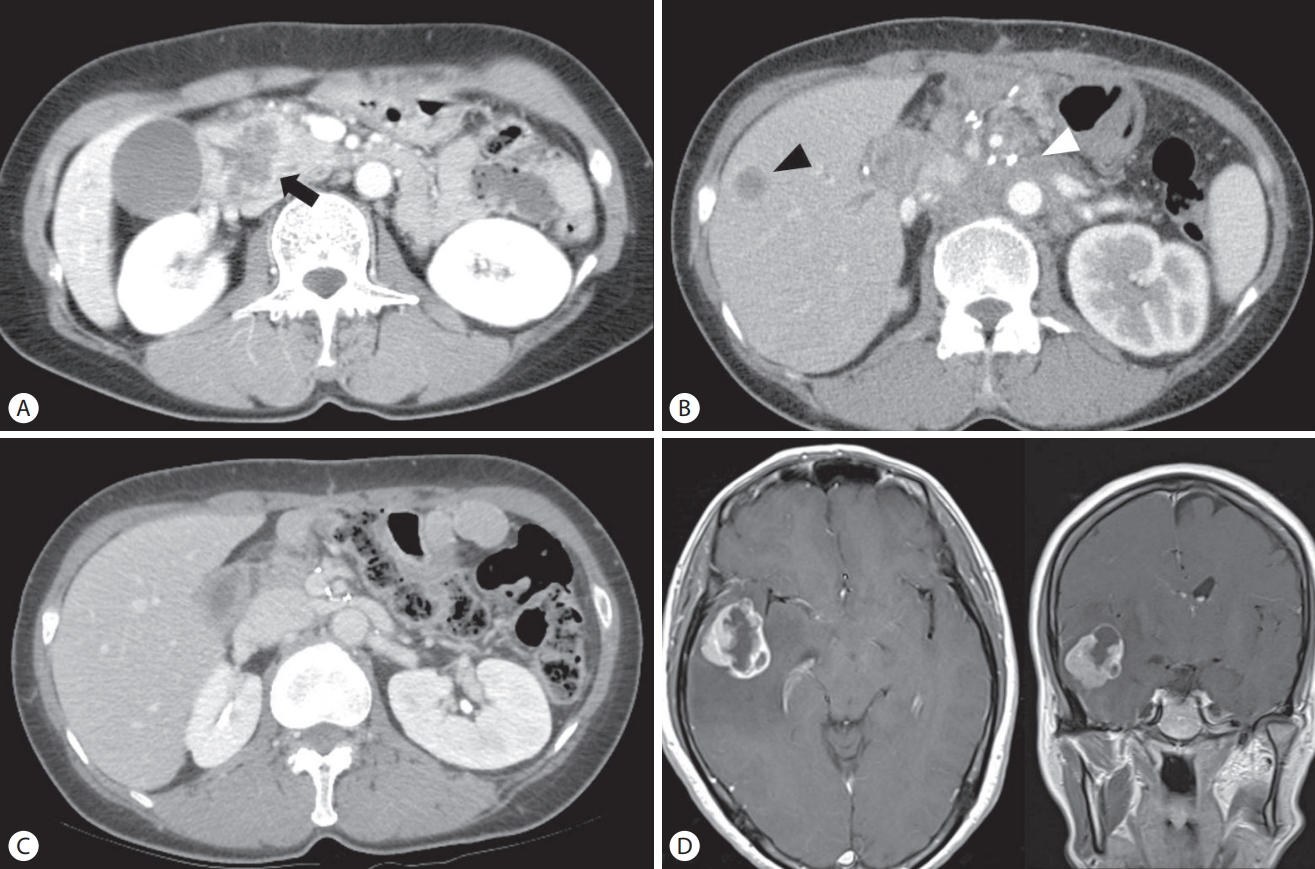
In May 2012, a 52-year-old woman presented with a week-long history of jaundice. Abdominal computed tomography (CT) revealed a 4.0 cm low-density mass at the head of the pancreas, which invaded the duodenum (Fig. 1A). Endoscopically, an ulcerofungating mass lesion was identified in the second portion of the duodenum, and a biopsy of the lesion revealed metastatic adenocarcinoma from the pancreas. Laboratory tests showed the following: bilirubin (total/direct), 12.0/8.0 mg/dL; aspartate transaminase/alanine transaminase, 168/315 U/L; alkaline phosphatase, 518 U/L; and gamma glutamyl transpeptidase, 632 U/L. The carbohydrate antigen 19–9 (CA 19–9) level was 2,758 U/mL.
After excluding distant metastasis using positron emission tomography, the patient underwent pylorus-preserving pancreaticoduodenectomy. The pathologic result of the operation revealed a poorly differentiated adenocarcinoma with lymph node metastases, and the American Joint Committee on Cancer (AJCC, 7th edition) stage was IIB. Thereafter, the patient received a total of three cycles of adjuvant chemotherapy (gemcitabine, 1,000 mg/m2 weekly for the first 3 weeks and then 1 week of rest). Follow-up abdominal CT revealed multiple new hepatic metastases (Fig. 1B), and secondary chemotherapy was administered using the XP regimen (capecitabine 1,000 mg/m2 twice daily on days 1–14, and cisplatin 60 mg/m2 on day 1, every 3 weeks) from October 2012 for a total of eight cycles to March 2013. A partial response based on the Revised Evaluation Criteria in Solid Tumors (RECIST) criteria was attained. Since April 2013, she was treated with only capecitabine (1,000 mg/m2 twice daily on days 1–14, every 3 weeks) because of emesis caused by cisplatin and poor performance status, and she had received a total of 11 cycles until October 2013. Follow-up abdominal CT revealed disappearance of all metastatic lesions in the liver (Fig. 1C).
In November 2013, she complained of a headache and transient paresthesia in the left leg. Although abdominal CT, which was performed 1 week prior to the presentation, indicated that she had achieved complete response, CA 19-9 level was elevated to 99.7 U/mL, compared to 13.3 U/mL detected 2 months prior. Brain magnetic resonance imaging (MRI) showed a 3.3 cm mass in the right temporal lobe (Fig. 1D). After 1 month, she was referred to the emergency department with headache, dizziness, and vomiting. She underwent a craniotomy and resection of the temporal lobe mass. Histological examination of the brain specimen revealed a metastatic adenocarcinoma (Fig. 2A, B), which was consistent with the primary pancreatic tumor based on immunohistochemical staining (Fig. 2C, D). Follow-up brain MRI showed small new metastases in the right frontal base and right occipital lobe, and she underwent gamma knife surgery in January 2014. Despite aggressive treatment, the neurological symptoms progressed and the patient died in April 2014.
DISCUSSION
Brain metastases are frequently diagnosed in patients with lung cancer (48%), breast cancer (15%), testicular cancer (10% to 15%), and malignant melanoma (6% to 10%). However, they rarely arise from gastrointestinal tract cancers [6]. Brain metastases are reported in < 4% of malignancies affecting the esophagus, stomach, colon, and rectum [7]. Brain metastases originating from pancreatic cancer are exceedingly rare, which have been reported in 0.33% of pancreatic adenocarcinoma cases [5]. This is attributed to the aggressive nature of pancreatic adenocarcinoma and the fact that most patients do not exhibit sufficiently long survival periods for tumor cells to invade the nervous system [5,8]. To the best of our knowledge, only 21 cases of brain metastases from pancreatic cancer identified antemortem have been reported to date, including our case. Table 1 summarizes the clinical features of these cases. Most patients have been men (17 men, 4 women), and brain metastases represented the first manifestation of pancreatic cancer in 6 patients. Prognosis was extremely poor, with the majority of patients dying within a year, most of them within weeks or months. Four patients survived for longer than 20 months, 36 months, 6 years, and 10 years, respectively, after the diagnosis of brain metastases [9-11].
In general, the treatment strategy for brain metastases from pancreatic cancer tends to be palliative due to the extremely poor prognosis. Treatments for metastatic brain tumors from pancreatic cancer have included surgical resection, whole-brain radiotherapy and stereotactic radiosurgery [8-15]. Given the radio-resistant nature of most pancreatic cancers, radiotherapy appears to offer little benefit [5,6]. In contrast, aggressive surgical resection may prove to be effective. Ten reports have described surgical resection for metastatic brain tumors from pancreatic cancer, including our case [8-15]. Survival periods were significantly longer in patients who underwent surgical resection than in patients who did not undergo resection.
In contrast to our case, Lemke et al. [9] reported two patients with long-term survival of more than 5 years after surgical resection. Based on a literature review of favorable survival in patients with brain metastases, curative therapy for pancreatic cancer was associated with long-term survival after a diagnosis of brain metastasis [14]. However, in our case, the survival period was relatively short (5 months), even though the patient received curative treatment for pancreatic cancer. This may be related to the fact that the patient refused treatment for brain metastasis at the time of its diagnosis, and that she was treated only after the symptoms deteriorated 1 month later. Although she had undergone resection for brain metastasis 1 month after the diagnosis, additional brain metastases were confirmed on postoperative imaging, suggesting that the timing of resection for brain metastasis was delayed.
In conclusion, we reported a case of brain metastasis from pancreatic cancer that showed favorable progress with palliative chemotherapy for 13 months. Brain metastasis should be considered in patients with pancreatic cancer presenting with new neurological symptoms.
Although the prognosis for patients with pancreatic cancer and brain metastasis is very poor, surgical resection of brain metastasis may allow for long-term survival in patients in whom the primary pancreatic cancer is well controlled. Therefore, surgical resection of brain metastases at the appropriate time may improve patient prognosis.